You’re three months postpartum. The sleep deprivation you expected. The emotional rollercoaster you prepared for. But the hair? Nobody warned you about this.
You run your fingers through your hair in the shower and pull out what looks like enough strands to knit a sweater. Your hairbrush is a crime scene. The drain is clogged again. And when you look in the mirror, your part line seems wider than it was last week.
This article contains affiliate links. See our affiliate disclosure for details.
Here’s what’s happening: you’re experiencing postpartum telogen effluvium, the medical term for the hair shedding that affects roughly 40-50% of women after childbirth. It’s triggered by the dramatic hormonal shift that occurs when estrogen levels plummet after delivery. During pregnancy, improved estrogen kept more of your hair follicles in the growth phase. Now they’re all catching up, entering the resting phase simultaneously, and shedding in what feels like alarming quantities.
But here’s the critical question: when is this normal, and when does it signal something more serious? Because while postpartum hair loss is common, it’s not always benign. And the difference between normal shedding and a condition that requires medical attention can be subtle. This guide will help you distinguish between the two, understand what’s actually happening to your hair follicles, and identify the evidence-based interventions that can help (and the popular remedies that won’t).
Understanding the Postpartum Hair Loss Timeline
Postpartum hair loss follows a predictable pattern, and understanding this timeline is crucial for knowing when your experience falls within normal parameters.
During pregnancy, your estrogen levels can increase by up to 100-fold. This hormonal surge has a profound effect on your hair growth cycle. Normally, about 85-90% of your hair follicles are in the anagen (growth) phase at any given time, with the remaining 10-15% in telogen (resting) phase before shedding. But during pregnancy, that percentage shifts dramatically. More follicles stay in the growth phase, fewer enter the resting phase, and your overall hair density increases.
This is why many women report having the best hair of their lives during pregnancy. It’s thicker, fuller, and seems to grow faster. You’re not imagining it. You genuinely have more hair on your head because less is falling out.
Then you give birth. Within 24 hours, your estrogen levels drop precipitously, returning to pre-pregnancy levels within about a week. This sudden hormonal shift signals to all those extra follicles that were hanging out in the growth phase that it’s time to move along. They enter the resting phase en masse.
Hair follicles don’t shed immediately upon entering telogen. There’s typically a 2-3 month lag between entering the resting phase and actual hair loss. This is why postpartum shedding usually begins around 3-4 months after delivery, peaks between 4-6 months, and gradually tapers off by 9-12 months postpartum.
According to research published in the Journal of the American Academy of Dermatology, women can lose between 300-500 hairs per day during peak postpartum shedding, compared to the normal 50-100 hairs daily. That’s a significant increase, but it’s also temporary and self-limiting in most cases.
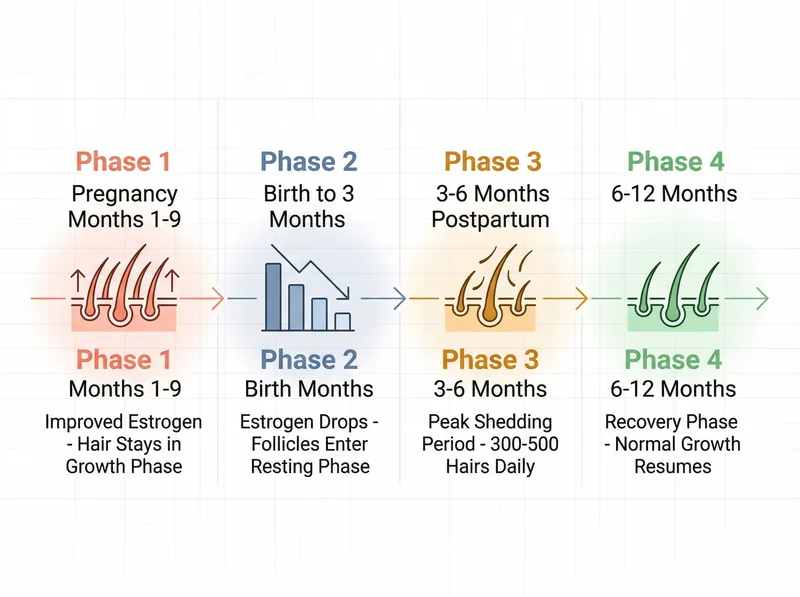 The typical timeline of postpartum hair loss, from hormonal changes during pregnancy to expected recovery periods.
The typical timeline of postpartum hair loss, from hormonal changes during pregnancy to expected recovery periods.
Red Flags: When Hair Loss Isn’t Normal
While postpartum telogen effluvium is common and usually resolves on its own, certain patterns suggest something more serious is happening. Here’s when you need to see a doctor.
First, timing matters. If your hair loss begins immediately after delivery or within the first month, that’s not typical postpartum shedding. Normal postpartum hair loss has that characteristic 2-3 month delay. Immediate hair loss could indicate a different condition, such as alopecia areata (an autoimmune condition) or severe nutritional deficiency.
Second, pattern matters. Postpartum telogen effluvium causes diffuse thinning, meaning hair loss is relatively even across your scalp, though it may be more noticeable at the temples and crown where hair is naturally finer. If you’re developing distinct bald patches, circular areas of complete hair loss, or asymmetric patterns, that’s not normal postpartum shedding. That could be alopecia areata or another form of scarring alopecia that requires immediate medical intervention.
Third, accompanying symptoms matter. Normal postpartum shedding doesn’t hurt. If you’re experiencing scalp pain, burning, itching, redness, scaling, or any kind of inflammation, something else is going on. These symptoms could indicate seborrheic dermatitis, scalp psoriasis, or a fungal infection, all of which require specific treatment.
Fourth, duration matters. If you’re still experiencing significant hair loss beyond 12 months postpartum, or if your hair density hasn’t begun to recover by 15-18 months, that warrants investigation. Prolonged hair loss could indicate an underlying condition that was unmasked by pregnancy, such as thyroid dysfunction, iron deficiency anemia, or androgenetic alopecia (pattern hair loss).
A study in the International Journal of Women’s Dermatology found that approximately 30% of women with persistent postpartum hair loss had an underlying thyroid disorder that went undiagnosed. Postpartum thyroiditis affects 5-10% of women and can cause either hyperthyroidism or hypothyroidism, both of which can trigger hair loss that extends well beyond the normal postpartum timeline.
If any of these red flags apply to you, don’t wait. Schedule an appointment with a dermatologist or trichologist who can perform a thorough scalp examination, pull test, and order appropriate blood work. Early intervention makes a significant difference in outcomes for most hair loss conditions.
 Key differences between normal postpartum shedding and hair loss patterns that warrant medical attention.
Key differences between normal postpartum shedding and hair loss patterns that warrant medical attention.
The Role of Nutritional Deficiencies
Pregnancy and breastfeeding create enormous nutritional demands. Your body prioritizes the baby, which means your hair follicles are often last in line for nutrients. And if you’re already running on empty, your hair will show it.
Iron deficiency is the most common nutritional culprit in postpartum hair loss. A study published in the Journal of Korean Medical Science found that women with serum ferritin levels below 40 ng/mL were significantly more likely to experience prolonged postpartum hair loss. The standard reference range for ferritin starts at 12-15 ng/mL, but for optimal hair growth, you want levels above 40, ideally between 70-80 ng/mL.
During pregnancy, your blood volume increases by 40-50%, which dilutes your iron stores. Then you lose blood during delivery. If you’re breastfeeding, you’re transferring iron to your baby through breast milk. And if your diet doesn’t include adequate iron-rich foods or you’re not absorbing iron efficiently, you can quickly become depleted.
But it’s not just iron. Zinc, biotin, vitamin D, and protein are all critical for hair growth, and all can become depleted during pregnancy and lactation. Zinc deficiency can cause telogen effluvium that looks identical to postpartum shedding but doesn’t resolve on its own. Biotin deficiency is rare but can occur in women who are breastfeeding and not supplementing. Vitamin D deficiency is extremely common in the Gulf region due to limited sun exposure and can affect hair follicle cycling.
Protein is particularly important because hair is made of keratin, a structural protein. If your protein intake is inadequate, your body will ration available protein for vital functions, and hair growth will be deprioritized. The World Health Organization recommends that lactating women consume an additional 19 grams of protein daily above baseline needs, but many women don’t meet even baseline requirements.
If you’re experiencing prolonged or severe postpartum hair loss, ask your doctor to check: serum ferritin (not just hemoglobin), zinc, vitamin D (25-hydroxyvitamin D), thyroid function (TSH, free T3, free T4), and possibly vitamin B12. These are the most common deficiencies associated with hair loss, and they’re all correctable with appropriate supplementation.
Environmental Factors in the Gulf Region
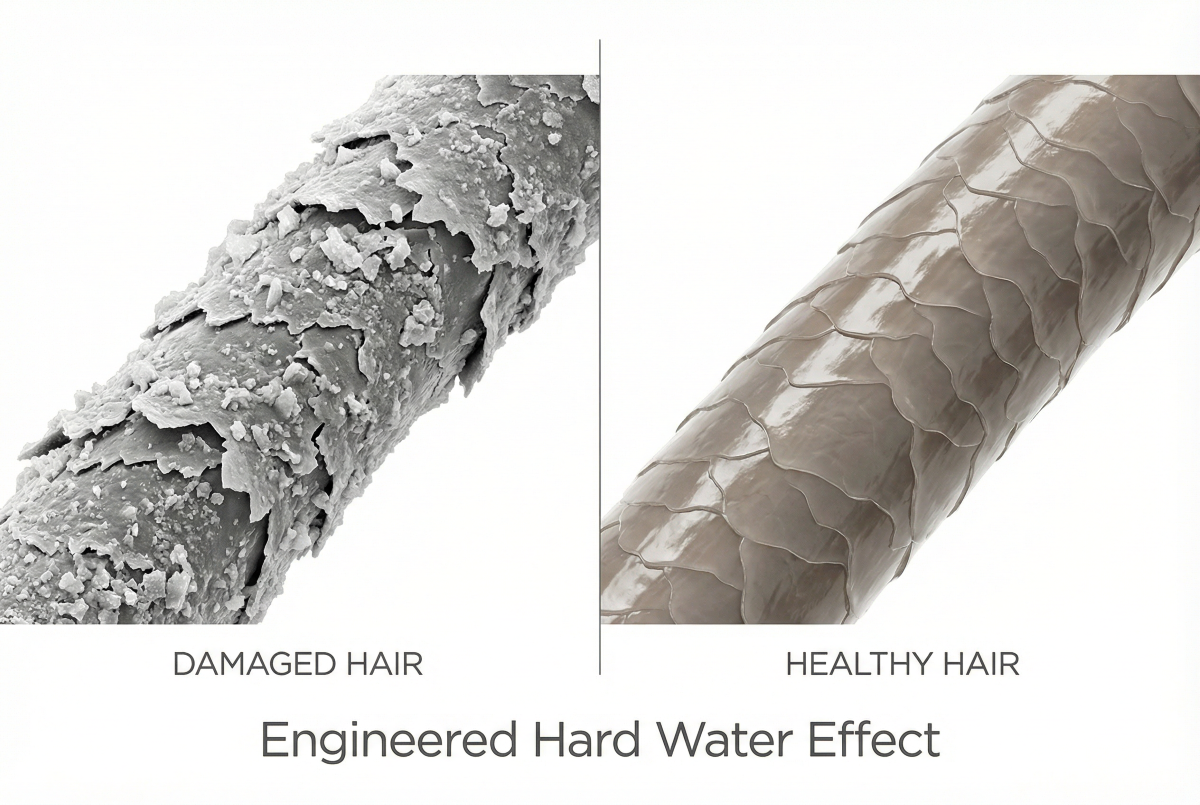
If you’re living in the Gulf region, there’s an additional factor affecting your postpartum hair recovery: water quality. The extremely hard water common throughout the Gulf can compound postpartum hair loss by creating mineral buildup on the scalp that impairs follicle function.
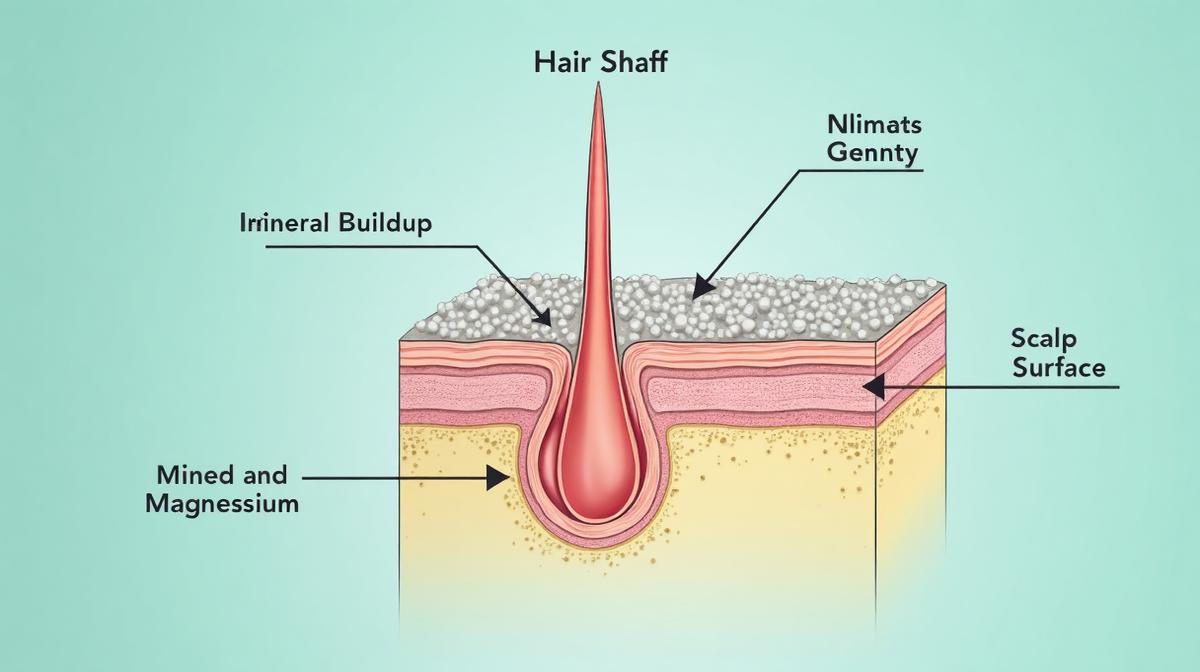
Hard water contains high concentrations of calcium and magnesium minerals. When you wash your hair, these minerals bond to the hair shaft and accumulate on the scalp, creating a barrier that prevents moisture from penetrating the hair and can clog follicles. For women already dealing with postpartum hormonal changes and potential nutritional deficiencies, this additional stress on the scalp can prolong recovery.
The issue is particularly pronounced in the Gulf because water hardness levels here often exceed 300 ppm (parts per million), compared to the 60 ppm threshold where water is considered ‘hard.’ This extreme mineral content creates a cumulative effect. Even if you’re using high-quality hair products and taking appropriate supplements, if you’re washing your hair in extremely hard water, you’re constantly depositing minerals that interfere with scalp health.
For women dealing with postpartum hair loss in the Gulf, addressing water quality is a critical but often overlooked component of recovery. Using a chelating shampoo like Regrowth+ once or twice weekly can help remove mineral buildup and restore normal scalp function, creating a better environment for hair regrowth. For more on how hard water affects hair health, see our guide on hard water and hair loss.
 Essential nutrients that support hair regrowth during the postpartum period and their best food sources.
Essential nutrients that support hair regrowth during the postpartum period and their best food sources.
What Actually Helps: Evidence-Based Interventions
Now for what you actually want to know: what can you do about it? Here’s what the science supports.
First, understand that normal postpartum telogen effluvium is self-limiting. Your hair will recover on its own as your hormones stabilize and your follicles reset their growth cycle. There is no treatment that will make postpartum shedding stop immediately because the hair that’s falling out has already been programmed to shed. It entered the resting phase months ago. What you can do is improve conditions for the new growth that’s coming in behind it.
Nutritional improvation is the single most important intervention. If you’re deficient in iron, zinc, vitamin D, or protein, no topical treatment will compensate. Address the deficiency first. Work with your doctor to correct any identified deficiencies with appropriate supplementation. For iron, ferrous sulfate or ferrous gluconate are well-absorbed forms. Take it with vitamin C and away from calcium, which inhibits absorption. For vitamin D, most postpartum women need 2000-4000 IU daily to achieve optimal levels. For zinc, 15-25 mg daily is typically sufficient.
Protein intake deserves special attention. Aim for 1.2-1.5 grams of protein per kilogram of body weight if you’re breastfeeding. That’s roughly 80-100 grams daily for most women. Distribute it across meals rather than loading it all at dinner. Your body can only process about 25-30 grams of protein at once for muscle and tissue synthesis.
Topical minoxidil is the only FDA-approved treatment for hair loss in women and can be used while breastfeeding (though you should discuss this with your doctor). A 2% minoxidil solution applied twice daily can accelerate the transition of follicles from telogen back to anagen, potentially shortening your recovery timeline. However, minoxidil is most effective for androgenetic alopecia (pattern hair loss) rather than telogen effluvium, so its benefit for postpartum shedding specifically is modest.
Scalp care matters more than most women realize. A healthy scalp environment supports hair regrowth. This means gentle cleansing with a sulfate-free shampoo, avoiding excessive heat styling, and addressing any scalp conditions like dandruff or seborrheic dermatitis that can impair follicle function. If you’re in the Gulf region, this also means managing hard water mineral buildup with periodic chelating treatments.
What doesn’t help: biotin supplements (unless you’re actually deficient, which is rare), collagen supplements (no evidence for hair growth), hair growth serums with peptides or stem cells (no clinical evidence), scalp massages (pleasant but not proven to affect hair density), and most importantly, stressing about it. Stress can prolong telogen effluvium by keeping follicles in the resting phase longer. Easier said than done when you’re looking at handfuls of hair, but understanding that this is temporary and normal can help reduce the anxiety that makes it worse.
Managing the Psychological Impact
The emotional toll of postpartum hair loss is real and often underestimated. You’re already navigating the enormous identity shift of becoming a mother, dealing with sleep deprivation, possible postpartum depression or anxiety, and now your hair is falling out. It’s a lot.
Research published in the International Journal of Trichology found that women with visible hair loss reported significantly higher rates of anxiety, depression, and reduced quality of life compared to women without hair loss. The psychological impact of hair loss is not superficial or vain. Hair is tied to identity, femininity, and self-image. Losing it during an already vulnerable time compounds the emotional challenges of the postpartum period.
If you’re struggling emotionally with postpartum hair loss, know that your feelings are valid. It’s okay to grieve the loss of your pre-pregnancy hair while simultaneously being grateful for your baby. These feelings can coexist. Consider talking to a therapist who specializes in postpartum issues if the hair loss is contributing to anxiety or depression.
Practical coping strategies can help. Consider a shorter haircut, which can make thinning less noticeable and reduce the visual impact of shedding. Use volumizing products at the roots. Try a different part line to disguise thinning at your usual part. If you’re comfortable with it, talk to other mothers about their experiences. You’ll likely find that many women have been through this and came out the other side with full hair recovery.
Set realistic expectations. Your hair probably won’t return to pre-pregnancy density and texture immediately. The regrowth phase can take 6-12 months, and the new hair coming in will initially be short and may have a different texture. Those short hairs sticking up around your hairline? That’s regrowth. It’s a good sign, even if it looks a bit odd for a while.
Most importantly, give yourself grace. You’re recovering from pregnancy and childbirth, possibly breastfeeding, definitely sleep-deprived, and adjusting to a massive life change. Your hair will recover. Your body is doing exactly what it’s supposed to do. And in a year, this will be a distant memory.
References
- Postpartum telogen effluvium: A systematic review - Journal of the American Academy of Dermatology
- Postpartum thyroiditis and hair loss in women - International Journal of Women’s Dermatology
- Serum ferritin and hair loss in women - Journal of Korean Medical Science
- Nutritional requirements during lactation - World Health Organization
- Psychological impact of hair loss in women - International Journal of Trichology