This article contains affiliate links. See our affiliate disclosure for details.
You’ve dealt with eczema on your hands, your elbows, maybe the backs of your knees. But when it reaches your scalp? That’s a different kind of misery. The itch is relentless. The flakes are embarrassing. And every shampoo you try seems to make it worse.
Here’s what most people don’t realize: scalp eczema (atopic dermatitis of the scalp) is fundamentally different from the dandruff or seborrheic dermatitis that most scalp treatments target. The skin barrier on your scalp is compromised in a specific way that makes standard anti-dandruff shampoos not just ineffective but actively irritating.
And if you’re in the Gulf region, there’s another factor making everything worse: the mineral content in your water. Research published in the Journal of Investigative Dermatology confirms that hard water changes the skin barrier and increases irritant penetration, exactly what eczema-prone skin can’t handle.
This isn’t another generic ‘try moisturizing more’ guide. We’re breaking down the actual pathophysiology of scalp eczema, why it’s so often misdiagnosed, and the specific treatment protocol that addresses the root barrier dysfunction. If you’ve been treating your scalp like it has dandruff when it actually has eczema, this explains why nothing’s worked.
Why Scalp Eczema Gets Misdiagnosed (And Why That Matters)
Walk into most clinics with an itchy, flaky scalp and you’ll walk out with a prescription for ketoconazole or selenium sulfide, antifungal treatments designed for seborrheic dermatitis. For scalp eczema, these are the wrong tools entirely.
The confusion is understandable. Both conditions cause flaking and redness. Both can itch intensely. But the underlying mechanisms are opposite. Seborrheic dermatitis involves excess oil production and an overgrowth of Malassezia yeast. Atopic dermatitis involves a dry, changeed skin barrier with immune system overreaction.
Treating eczema with harsh antifungal shampoos is like trying to put out a fire with gasoline. The surfactants strip away what little protective lipid layer remains. The active ingredients irritate already-inflamed skin. You end up in a cycle where the ‘treatment’ perpetuates the problem.
The visual differences are subtle but diagnostic. According to the American Academy of Dermatology, atopic dermatitis on the scalp typically presents as dry, fine white flakes with diffuse redness, often concentrated along the hairline and behind the ears. Seborrheic dermatitis produces greasy, yellowish scales primarily on the crown and along the part line.
If you’ve had eczema elsewhere on your body, especially if it started in childhood, and you’re now dealing with scalp symptoms, atopic dermatitis is the more likely culprit. The genetic barrier defects that cause eczema don’t skip your scalp just because there’s hair there.
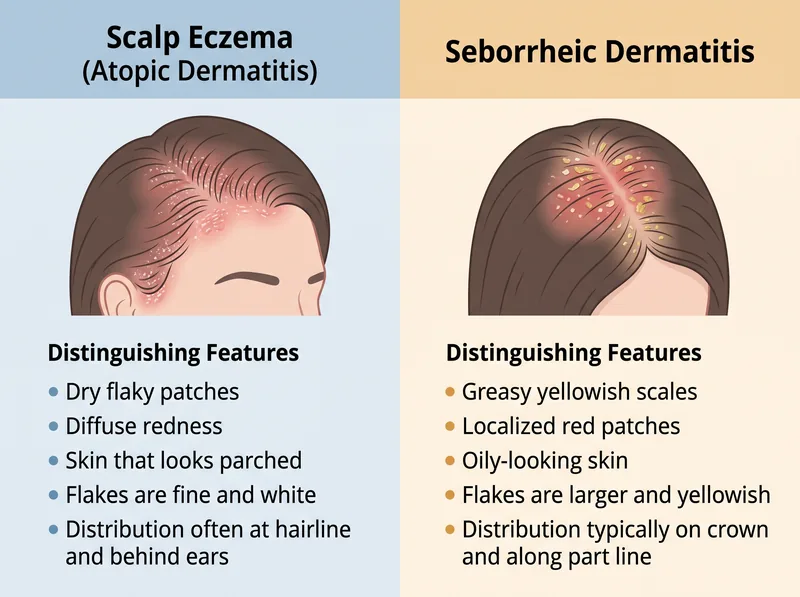 Key visual differences between atopic dermatitis and seborrheic dermatitis on the scalp, knowing which you have changes everything about treatment.
Key visual differences between atopic dermatitis and seborrheic dermatitis on the scalp, knowing which you have changes everything about treatment.
The Barrier Breakdown: What’s Actually Happening on Your Scalp
Your skin barrier is a brick-and-mortar structure. The ‘bricks’ are corneocytes (dead skin cells). The ‘mortar’ is a lipid matrix made of ceramides, cholesterol, and fatty acids. In atopic dermatitis, this mortar is defective.
Research in the Journal of Allergy and Clinical Immunology identified mutations in the filaggrin gene, the protein responsible for organizing the barrier structure, in a significant percentage of eczema patients. Without functional filaggrin, the barrier can’t hold together properly.
On your scalp, this defective barrier has two consequences. First, it can’t retain water effectively, leading to chronic dryness and the characteristic fine flaking. Second, it can’t keep irritants out, making your scalp hyperreactive to substances that wouldn’t bother normal skin.
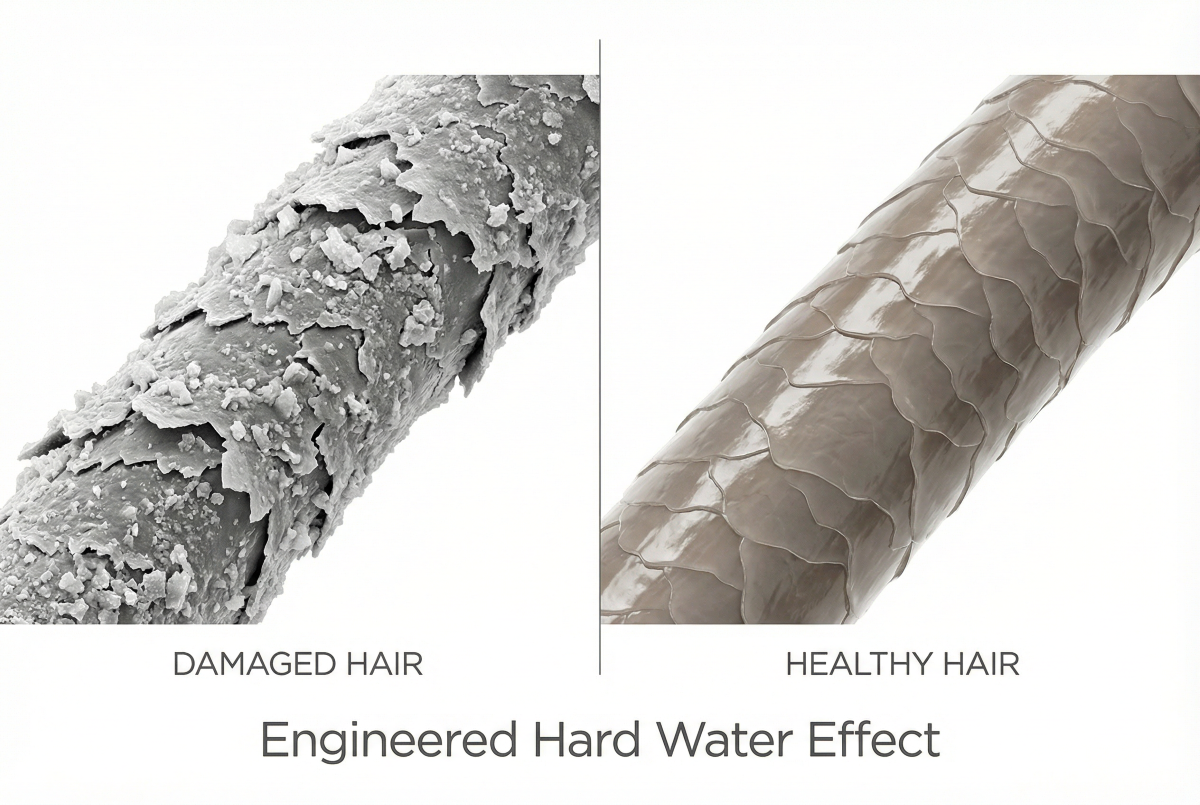
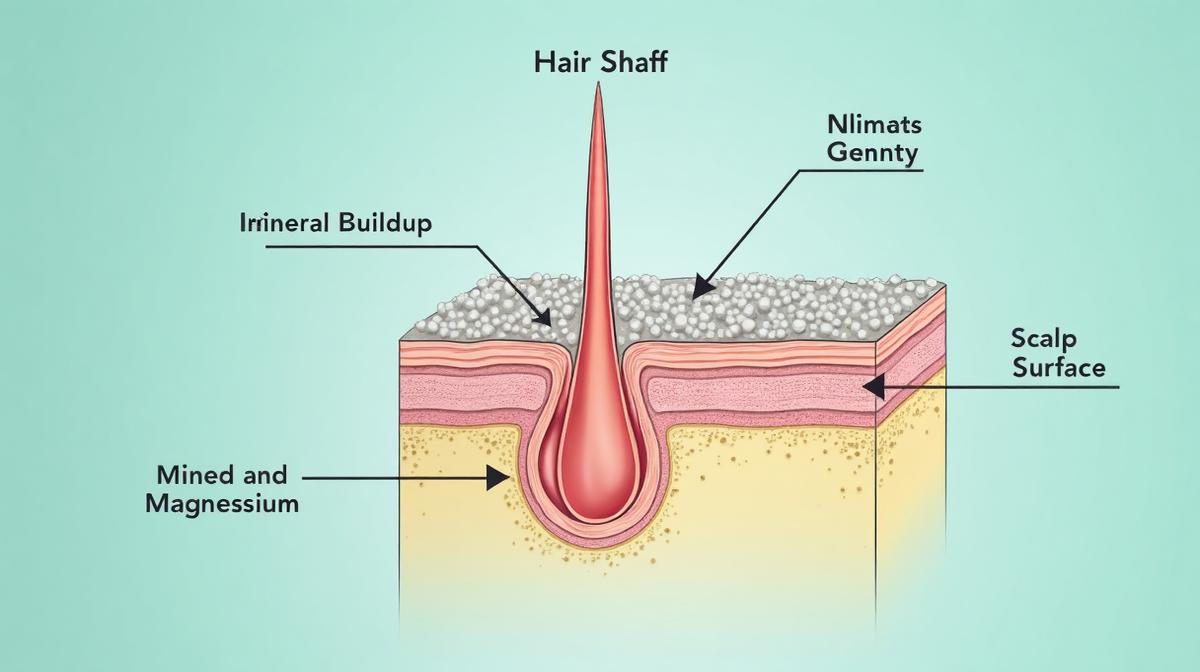
This is where the Gulf’s water quality becomes directly relevant. Hard water, defined as water with high concentrations of dissolved calcium and magnesium, interacts with soap to form an insoluble residue. This residue deposits on the scalp, and through a compromised eczema barrier, those minerals penetrate deeper into the skin.
A study in the Journal of Investigative Dermatology demonstrated that hard water exposure increased transepidermal water loss and improved levels of inflammatory markers in the skin. For someone with an already-defective barrier, hard water isn’t just an inconvenience, it’s a documented aggravating factor that perpetuates inflammation.
The immune component compounds the problem. In eczema, the immune system misidentifies harmless substances as threats, triggering inflammation. The more the barrier is changeed, the more antigens penetrate, the more the immune system overreacts. It’s a self-perpetuating cycle that standard dandruff treatments don’t address.
Environmental Triggers Specific to Gulf Residents
If your scalp eczema started or worsened after moving to the Gulf region, you’re not imagining the connection. The environmental factors here create a perfect storm for barrier-compromised skin.
The water chemistry is the primary culprit. According to the US Geological Survey, water hardness above 180 mg/L is classified as ‘very hard.’ Municipal water in many Gulf cities exceeds 300 mg/L, well into the severe hardness category.
Every time you shower, you’re coating your scalp with mineral deposits. For healthy skin, this might cause mild dryness. For eczema-prone skin with a defective barrier, it’s a continuous source of irritation. The minerals don’t rinse away cleanly, they bind to hair proteins and scalp tissue, creating a layer that traps irritants and prevents moisture from entering.
The climate adds another layer of stress. Low humidity means higher transepidermal water loss. Air conditioning creates rapid temperature and humidity fluctuations. Both stress the barrier’s ability to maintain hydration, and a dehydrated barrier is a more permeable barrier.
Indoor allergens are often overlooked. Dust mites thrive in the Gulf’s climate, and research in Clinical and Experimental Allergy shows that dust mite allergen exposure worsens atopic dermatitis through both barrier changeion and immune activation. Your scalp is exposed to these allergens every time you sleep on your pillow.
For anyone managing scalp eczema in this environment, addressing water quality isn’t optional, it’s a necessary part of the treatment protocol. A chelating shampoo like Regrowth+ removes the mineral buildup that standard shampoos leave behind, giving barrier-repair treatments a clean surface to work on.
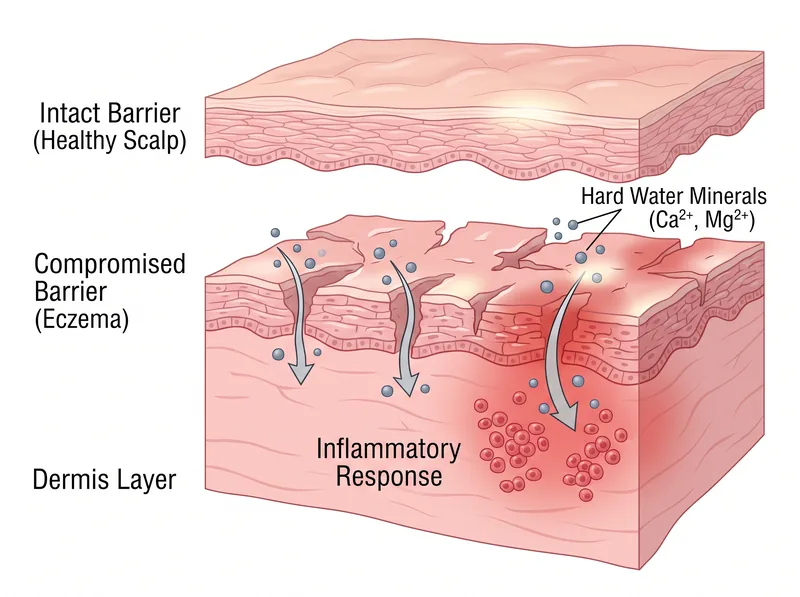 Hard water minerals penetrate the already-compromised barrier of eczema-affected scalp, triggering inflammation that healthy skin could resist.
Hard water minerals penetrate the already-compromised barrier of eczema-affected scalp, triggering inflammation that healthy skin could resist.
The Clinical Treatment Protocol That Actually Works
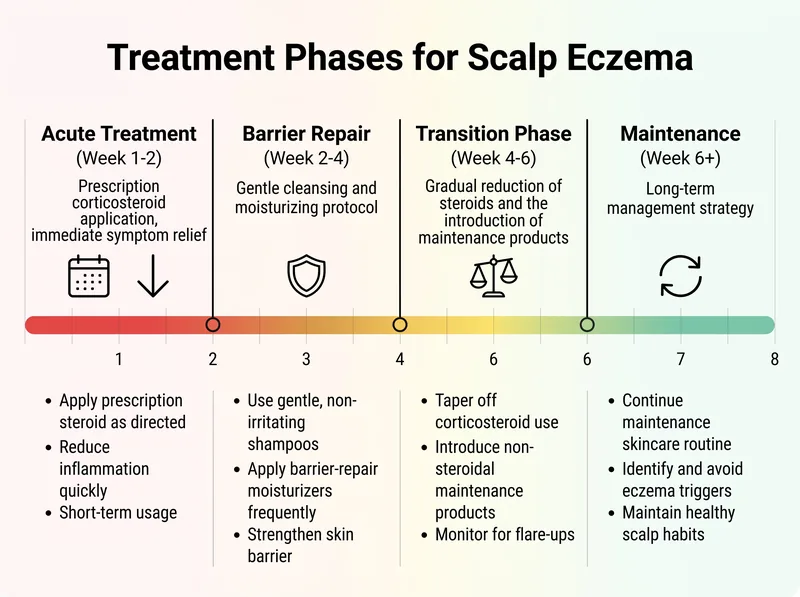
Effective scalp eczema treatment follows a structured protocol, not a random trial of products. The goal is threefold: suppress active inflammation, repair the barrier, then maintain remission. Skipping steps or doing them out of order is why most people fail to achieve lasting control.
Phase one is acute inflammation control. This requires prescription-strength topical corticosteroids, usually a solution or foam formulation designed for scalp application. Mayo Clinic guidelines recommend starting with a mid-to-high potency steroid applied once or twice daily until symptoms improve, typically 7-14 days.
The steroid isn’t treating the underlying cause, it’s buying you time by shutting down the inflammatory cascade. This allows the barrier to start healing without constant immune interference. But steroids alone don’t fix the barrier defect, which is why they fail as monotherapy.
Phase two begins as inflammation subsides: barrier repair. This means introducing lipid-rich moisturizers that contain the specific components eczema skin lacks. Look for formulations with ceramides, cholesterol, and fatty acids in a 3:1:1 ratio, the optimal ratio for barrier restoration according to dermatology research.
For the scalp specifically, this is tricky. Heavy creams don’t work well on hair-bearing skin. You need lightweight serums or sprays that deliver barrier-repair lipids without leaving residue. Apply these to the scalp (not the hair) after washing, while the skin is still slightly damp to trap moisture.
Phase three is the steroid taper. You can’t use topical steroids indefinitely, they cause skin thinning and rebound inflammation when stopped abruptly. The protocol is to gradually reduce frequency: daily to every other day to twice weekly, while maintaining the barrier-repair routine. Some patients transition to topical calcineurin inhibitors (tacrolimus or pimecrolimus) for long-term control without steroid side effects.
Phase four is maintenance, and this is where water quality management becomes critical. Even after achieving remission, continuing to shower in hard water will slowly re-damage the barrier. The maintenance protocol includes: gentle, sulfate-free cleansing with chelating properties to remove mineral buildup, regular application of barrier-repair moisturizers, and avoidance of known triggers (harsh shampoos, excessive heat styling, irritating hair products).
This isn’t a two-week fix. Expect 4-6 weeks to see significant improvement, and understand that scalp eczema is a chronic condition requiring ongoing management. But with the right protocol, most patients achieve sustained remission with minimal maintenance therapy.
 The realistic timeline for scalp eczema improvement, most people see barrier repair within 2-3 weeks, but full control takes consistent maintenance.
The realistic timeline for scalp eczema improvement, most people see barrier repair within 2-3 weeks, but full control takes consistent maintenance.
What to Avoid (These Make Everything Worse)
Knowing what not to do is as important as knowing what to do. Several common practices actively sabotage scalp eczema treatment, often because they’re recommended for other scalp conditions.
Stop using dandruff shampoos with zinc pyrithione, selenium sulfide, or coal tar. These are designed for seborrheic dermatitis and psoriasis, conditions with excess cell turnover and fungal involvement. For eczema’s dry, compromised barrier, they’re too harsh. The surfactants strip lipids, the active ingredients irritate inflamed skin, and you end up worse than you started.
Avoid sulfates, particularly sodium lauryl sulfate (SLS) and sodium laureth sulfate (SLES). These are powerful detergents that remove oil efficiently, too efficiently for eczema skin. Research in Contact Dermatitis showed that SLS significantly increases transepidermal water loss and skin irritation, especially in individuals with compromised barriers.
Don’t over-wash. The instinct when your scalp is flaking is to wash more frequently, thinking you need to remove the flakes. But frequent washing strips the scalp’s natural oils, worsening dryness and barrier dysfunction. For most people with scalp eczema, washing 2-3 times per week is sufficient once inflammation is controlled.
Skip the hot water. High water temperature feels soothing on itchy skin, but it damages the lipid barrier and increases inflammation. Lukewarm water only, yes, even in the Gulf’s climate where a cold shower sounds appealing. Temperature extremes stress already-compromised skin.
Eliminate fragranced products. Fragrance is one of the most common contact allergens, and eczema skin is hyperreactive to allergens. Even ‘natural’ fragrances from essential oils can trigger flares. If a product lists ‘fragrance’ or ‘parfum’ in the ingredients, it’s not suitable for eczema management.
Don’t scratch. This seems obvious, but the itch-scratch cycle is a major perpetuator of eczema. Scratching damages the barrier further, allows more allergen penetration, triggers more inflammation, causes more itching. If nighttime scratching is an issue, consider cotton gloves while sleeping and keep nails trimmed short.
When to See a Dermatologist (Don’t Wait Too Long)
Some scalp conditions require professional diagnosis and prescription treatment. Self-management has limits, and knowing when you’ve reached them prevents months of ineffective trial and error.
See a dermatologist if over-the-counter eczema treatments haven’t improved symptoms within 2-3 weeks. Persistent inflammation needs prescription-strength intervention. Delaying treatment allows the condition to worsen and can lead to secondary complications like bacterial infection.
Seek immediate evaluation if you notice oozing, crusting, or honey-colored discharge. These are signs of secondary bacterial infection (usually Staphylococcus aureus), which is common in eczema due to the compromised barrier. Infected eczema requires antibiotic treatment in addition to anti-inflammatory therapy.
Get professional assessment if the flaking is accompanied by thick, silvery scales or well-defined red plaques. This suggests psoriasis rather than eczema, and the treatment approach is different. Psoriasis often requires phototherapy or systemic medications that eczema doesn’t need.
Consult a specialist if you’re experiencing significant hair loss along with scalp symptoms. While eczema itself doesn’t cause permanent hair loss, severe inflammation can change the hair growth cycle and lead to temporary shedding. Persistent hair loss may indicate a scarring alopecia that requires different treatment.
Don’t attempt to manage severe, widespread scalp eczema without medical supervision. If the affected area covers more than 30% of your scalp, or if symptoms are significantly impacting your quality of life (sleep changeion, anxiety, social avoidance), you need a dermatologist’s expertise and likely prescription medications.
References
- Hard Water Exposure and Skin Barrier Function - Journal of Investigative Dermatology
- Atopic Dermatitis: Diagnosis and Treatment - American Academy of Dermatology
- Filaggrin Mutations and Atopic Dermatitis - Journal of Allergy and Clinical Immunology
- Water Hardness Classification - US Geological Survey
- Dust Mite Allergens and Atopic Dermatitis - Clinical and Experimental Allergy
- Atopic Dermatitis Treatment Guidelines - Mayo Clinic
- Sodium Lauryl Sulfate and Skin Barrier Changeion - Contact Dermatitis