Most hair loss is temporary. The follicle goes dormant, then wakes up months later. You shed, you wait, you regrow. But scarring alopecia doesn’t follow that script.
With cicatricial alopecia, inflammation destroys the hair follicle completely. The stem cells die. Scar tissue fills the space where the follicle used to be. And once that happens, nothing grows back. Ever.
Here’s the thing: early scarring alopecia looks deceptively similar to other scalp conditions. You might dismiss the redness as dandruff. The itching as stress. The thinning as normal shedding. By the time the scarring becomes obvious, you’ve already lost follicles you can’t recover.
This isn’t about vanity. It’s about preserving what you still have. Because the only treatment that works is catching it early, stopping the inflammation, and preventing further damage. Miss that window, and the loss becomes permanent.
If you’re noticing unusual scalp symptoms in the Gulf region, burning, tenderness, patchy thinning with smooth skin underneath, this is what you need to know about scarring alopecia, how it differs from reversible hair loss, and why immediate professional evaluation isn’t optional.
What Makes Scarring Alopecia Different From Other Hair Loss
The defining feature of cicatricial alopecia is permanent follicle destruction. In conditions like alopecia areata, the immune system attacks follicles but doesn’t kill them. The follicle shrinks, goes dormant, and can potentially recover. With scarring alopecia, the follicle is replaced by fibrous scar tissue.
Under a microscope, healthy scalp tissue shows intact follicular units with sebaceous glands, stem cell reservoirs, and clear follicle openings. Scarred tissue shows none of that. Just collagen fibers where follicles used to be.
Clinically, this means the affected areas feel different. Run your fingers over a patch of scarring alopecia and you’ll notice the skin is smooth, shiny, and completely devoid of the tiny bumps that mark follicle openings. There’s no peach fuzz. No miniaturized hairs trying to grow. Nothing.
The scarring can happen quickly or slowly depending on the type. Some forms progress over months. Others take years. But the end result is the same: once the follicle is gone, no treatment, not minoxidil, not finasteride, not PRP, not stem cells, will bring it back.
That’s why dermatologists treat scarring alopecia with such urgency. You’re not trying to regrow hair. You’re trying to stop the inflammatory process before it destroys more follicles. The hair you save is the hair you keep.
 The four primary categories of cicatricial alopecia each present with distinct patterns and progression rates
The four primary categories of cicatricial alopecia each present with distinct patterns and progression rates
Primary Scarring Alopecia: When the Follicle Is the Target
Primary cicatricial alopecias are conditions where the hair follicle itself is the primary target of inflammation. The immune system or an inflammatory process directly attacks follicular structures, leading to their destruction and replacement with scar tissue.
The most common types include lichen planopilaris, frontal fibrosing alopecia (a variant of lichen planopilaris), central centrifugal cicatricial alopecia, and discoid lupus erythematosus. Each has distinct patterns and demographics.
Lichen planopilaris typically presents with scattered patches of hair loss, often on the crown or sides of the scalp. Patients describe intense itching, burning, or tenderness around affected areas. The hair loss progresses in an irregular pattern, and close examination reveals redness and scale at the base of remaining hairs.
Frontal fibrosing alopecia causes recession of the frontal hairline and eyebrows, creating a band of smooth, pale skin along the forehead. It’s more common in postmenopausal women and has increased dramatically in prevalence over the past two decades for reasons researchers don’t fully understand.
Central centrifugal cicatricial alopecia starts at the crown and spreads outward in a centrifugal pattern. It disproportionately affects women of African descent and has been linked to certain hairstyling practices, though the exact trigger remains debated. The affected area shows decreased follicle density with a shiny, atrophic appearance.
Discoid lupus erythematosus causes well-demarcated patches of scarring alopecia, often with significant inflammation, hyperpigmentation at the borders, and scale. It can occur on the scalp even without systemic lupus symptoms, making it a localized autoimmune condition targeting the skin and follicles.
What these conditions share is irreversible follicular damage if left untreated. The inflammation must be suppressed quickly to prevent progression.
 Recognizing these early warning signs can mean the difference between treatable inflammation and permanent follicle loss
Recognizing these early warning signs can mean the difference between treatable inflammation and permanent follicle loss
Early Warning Signs You Shouldn’t Ignore
Scarring alopecia rarely announces itself clearly. The early signs are subtle and easily confused with more benign scalp conditions. But there are patterns that should trigger immediate concern.
First: persistent scalp symptoms that don’t respond to standard treatments. If you’ve been treating what you think is dandruff or seborrheic dermatitis for weeks with no improvement, or if the symptoms are getting worse, that’s a red flag. Scarring alopecia often presents with scale, redness, and inflammation that looks superficially similar to seborrheic dermatitis, but it doesn’t improve with antifungal shampoos or topical steroids alone.
Second: unusual sensations. Burning, stinging, or tenderness in specific areas of the scalp, especially if it’s localized rather than diffuse, can indicate follicular inflammation. Many patients describe a feeling of tightness or pain when touching the affected area. This isn’t the generalized scalp sensitivity you might get from a sunburn or product irritation. It’s focused and persistent.
Third: changes in hair texture or breakage patterns. Hairs in affected areas may become brittle and break off close to the scalp. You might notice that certain patches feel rougher or the hair seems coarser than surrounding areas. This happens because the inflammatory process damages the hair shaft as it emerges from the diseased follicle.
Fourth: the skin itself looks different. Even before obvious hair loss occurs, the scalp may appear shinier or smoother in certain spots. You might notice decreased visibility of follicle openings, the tiny dots where individual hairs emerge. This is one of the earliest signs that follicles are being destroyed.
Fifth: hair loss that doesn’t follow typical patterns. Unlike male or female pattern baldness, which follows predictable distributions, scarring alopecia often creates irregular patches. The borders may be well-defined or diffuse, but the loss doesn’t match the usual frontal recession or crown thinning you’d expect from androgenetic alopecia.
If you’re experiencing any combination of these symptoms, don’t wait. Scarring alopecia is a dermatologic emergency. Every week you delay is another week of potential follicle destruction.
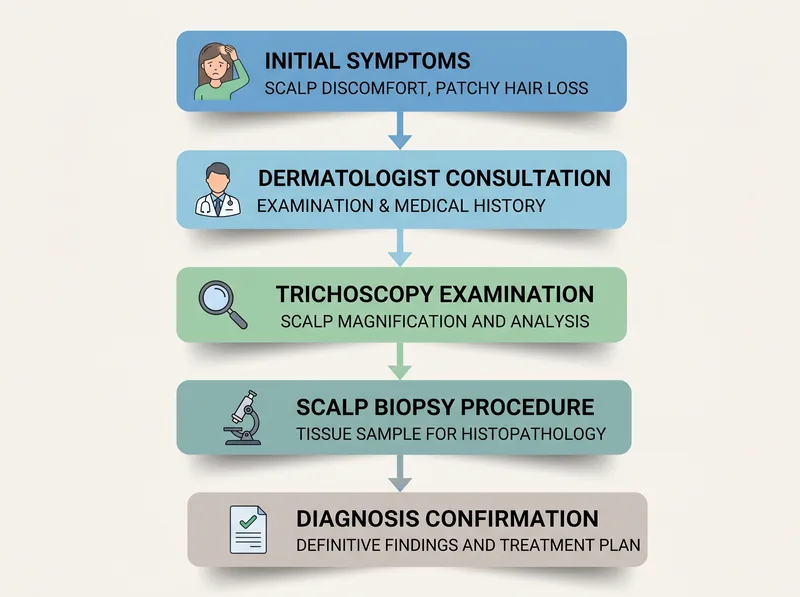 The diagnostic process for cicatricial alopecia requires specialist evaluation and often includes scalp biopsy for definitive diagnosis
The diagnostic process for cicatricial alopecia requires specialist evaluation and often includes scalp biopsy for definitive diagnosis
How Dermatologists Diagnose Cicatricial Alopecia
Diagnosis begins with clinical examination, but it doesn’t end there. A dermatologist will first assess the pattern and distribution of hair loss, examine the scalp surface for signs of inflammation or scarring, and look for the characteristic smooth, shiny appearance of affected areas.
Trichoscopy, examination of the scalp under high magnification, reveals features invisible to the naked eye. In scarring alopecia, trichoscopy typically shows absence of follicular openings in affected areas, perifollicular scaling, and often a distinctive pattern of redness or white dots where follicles have been replaced by scar tissue.
But the definitive diagnosis requires a scalp biopsy. This involves removing a small cylindrical sample of scalp tissue (usually 4mm in diameter) from an affected area. The sample is processed and examined under a microscope by a dermatopathologist.
The biopsy reveals what’s happening at the follicular level: the type and location of inflammation, the degree of follicular destruction, the presence of scar tissue, and specific features that distinguish one type of scarring alopecia from another. For example, lichen planopilaris shows a characteristic lymphocytic infiltrate around the upper follicle, while discoid lupus shows interface dermatitis and basement membrane thickening.
The biopsy also rules out other conditions. Certain infections, like fungal scalp infections or folliculitis decalvans, can cause scarring but require different treatments. The histopathology confirms the diagnosis and guides therapy.
Blood work may be ordered to check for underlying autoimmune conditions, especially if discoid lupus is suspected. A complete blood count, antinuclear antibody test, and other immunologic markers help determine if the scarring alopecia is part of a systemic disease or a localized scalp condition.
The entire diagnostic process, from initial consultation to biopsy results, typically takes two to three weeks. During that time, many dermatologists will start empiric anti-inflammatory treatment to prevent further follicle loss while awaiting confirmation.
Treatment Approaches: Stopping Inflammation Before It’s Too Late
There’s no cure for scarring alopecia. Once follicles are destroyed, they’re gone. Treatment focuses entirely on halting the inflammatory process to preserve remaining follicles. Speed matters.
First-line therapy typically involves topical or intralesional corticosteroids. These powerful anti-inflammatory medications suppress the immune response attacking the follicles. Intralesional injections, where the steroid is injected directly into the affected scalp areas, deliver high concentrations to the site of inflammation with minimal systemic absorption.
For more extensive or aggressive disease, oral immunosuppressants may be necessary. Hydroxychloroquine (commonly used for lupus), mycophenolate mofetil, or oral corticosteroids can provide systemic control of inflammation. These medications carry more significant side effects and require regular monitoring, but they may be the only option for rapidly progressive cases.
Topical calcineurin inhibitors like tacrolimus have shown benefit in some types of scarring alopecia, particularly lichen planopilaris. They work by suppressing T-cell activation and reducing inflammatory cytokine production at the follicular level.
Tetracycline antibiotics, particularly doxycycline, are often prescribed not for their antimicrobial effects but for their anti-inflammatory properties. They can help reduce follicular inflammation and are generally well-tolerated for long-term use.
The challenge is that treatment response varies dramatically between individuals. Some patients achieve complete disease control with topical steroids alone. Others require multiple medications and still experience slow progression. There’s no way to predict who will respond to what.
Treatment is typically continued for months to years, even after symptoms resolve, because scarring alopecia can reactivate. Many patients require maintenance therapy indefinitely to prevent flares.
One critical point: treatments like minoxidil or finasteride, which work for androgenetic alopecia, have no role in scarring alopecia. They can’t regrow hair from destroyed follicles, and they don’t address the underlying inflammatory process. Using them is a waste of time and money.
For areas with complete scarring and no remaining follicles, the only option for cosmetic restoration is hair transplantation, but this can only be considered after the disease has been inactive for at least one to two years. Transplanting into active inflammatory tissue will result in graft loss and potentially worsen the condition.
Environmental and Lifestyle Factors in the Gulf Region
While scarring alopecia is primarily an inflammatory or autoimmune condition, environmental factors in the Gulf region may influence disease expression and severity.
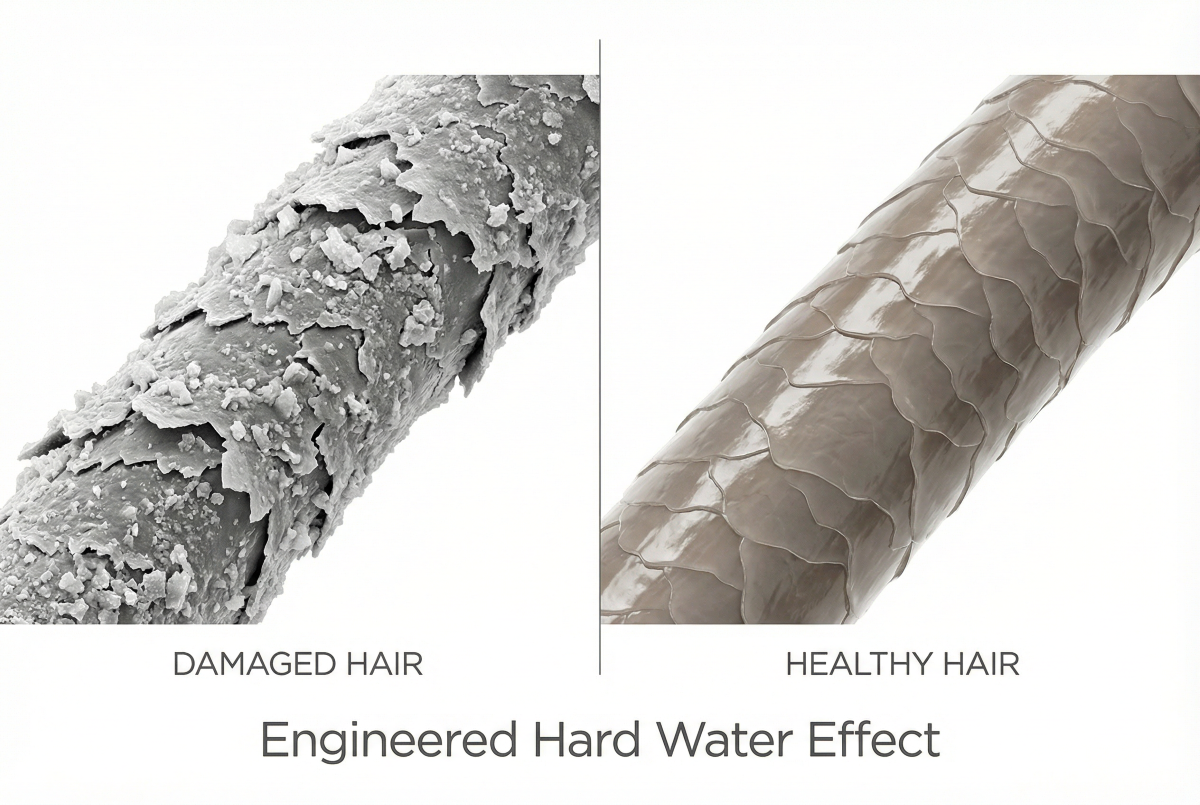
The intense heat and humidity can exacerbate scalp inflammation. Sweating increases moisture at the scalp surface, which can promote bacterial colonization and worsen follicular inflammation. Patients with active scarring alopecia often report that symptoms flare during summer months.
Hard water in the Gulf doesn’t cause scarring alopecia, but mineral buildup can irritate an already inflamed scalp. For patients undergoing treatment, using a chelating shampoo like Regrowth+ to remove mineral deposits may reduce additional scalp irritation, though it won’t address the underlying disease process.
Certain hairstyling practices common in the region, tight braiding, extensions, chemical relaxers, have been implicated in central centrifugal cicatricial alopecia, though the relationship is complex. It’s not that these practices directly cause the condition, but they may trigger or accelerate it in genetically predisposed individuals. The mechanical stress and chemical damage can initiate an inflammatory cascade that, in susceptible people, progresses to follicular destruction.
UV exposure is another consideration. The scalp receives significant sun exposure in the Gulf, and UV radiation can worsen inflammation in conditions like discoid lupus. Patients with active disease should protect their scalp with hats or UV-blocking sprays, especially in affected areas where hair coverage is reduced.
Stress, both psychological and physiological, appears to trigger flares in autoimmune conditions, including scarring alopecia. The high-stress lifestyle common among Gulf residents and expats may play a role in disease activation or progression, though this is difficult to quantify.
None of these factors alone cause scarring alopecia, but they can influence disease behavior in people who are already predisposed. Managing them won’t cure the condition, but it may help improve treatment outcomes.
Living With Scarring Alopecia: What to Expect Long-Term
A scarring alopecia diagnosis changes your relationship with your hair permanently. Even with successful treatment, you’re managing a chronic condition, not curing it.
Disease activity can fluctuate. You might achieve months or years of stability, then experience a flare triggered by stress, illness, or no identifiable cause. This unpredictability is one of the most challenging aspects psychologically. You can’t let your guard down.
Regular dermatology follow-up is essential. Most patients need appointments every three to six months to monitor disease activity, assess treatment response, and adjust medications. These visits typically include trichoscopy to detect early signs of reactivation before symptoms become obvious.
The cosmetic impact varies widely. Some patients lose only small patches that are easily concealed with hairstyling. Others experience extensive loss that significantly affects appearance and self-esteem. Hair systems, topical camouflage products, and strategic hairstyling can help, but they don’t address the underlying grief many people feel about permanent hair loss.
Mental health support is often necessary. The psychological impact of losing hair, especially when it’s permanent and progressive, can be profound. Anxiety about disease progression, depression related to appearance changes, and social withdrawal are common. Connecting with support groups or working with a therapist who understands chronic illness can make a significant difference.
For women, scarring alopecia can be particularly isolating. Hair loss in women carries different social stigma than in men, and the visible nature of scalp scarring can’t always be hidden. Many patients describe feeling invisible or judged, especially in cultures where female hair is closely tied to femininity and beauty.
The financial burden is also real. Medications, frequent dermatology visits, scalp biopsies, and cosmetic camouflage products add up. Many treatments aren’t fully covered by insurance, especially if they’re considered off-label use.
But here’s what patients who manage scarring alopecia successfully have in common: they treat it as a medical condition requiring ongoing management, not a cosmetic problem to fix and forget. They build a relationship with a dermatologist who understands cicatricial alopecias. They stay vigilant about symptoms. And they give themselves permission to grieve what they’ve lost while focusing on preserving what remains.
When to Seek Emergency Evaluation
Certain situations require immediate dermatologic evaluation, not a wait-and-see approach.
If you develop sudden, painful scalp lesions with rapid hair loss, especially if accompanied by pustules, crusting, or discharge, you need to be seen urgently. This could indicate folliculitis decalvans or dissecting cellulitis, aggressive forms of scarring alopecia that can destroy large areas of follicles in weeks without treatment.
Rapidly expanding patches of hair loss with intense inflammation, burning, or bleeding require prompt evaluation. The faster the progression, the more urgent the need for intervention.
If you’re already being treated for scarring alopecia and you notice sudden worsening despite medication compliance, contact your dermatologist immediately. This could indicate treatment failure, disease progression, or a secondary infection that needs to be addressed.
Don’t wait for your next scheduled appointment if you’re experiencing new symptoms. Scarring alopecia doesn’t follow a predictable timeline, and early intervention during a flare can prevent permanent damage.
For patients in the Gulf region, access to specialized dermatologists with trichology expertise may be limited outside major cities. If your local dermatologist isn’t familiar with scarring alopecia, ask for a referral to a specialist or seek a second opinion at a larger medical center. The stakes are too high to work with someone who doesn’t have experience managing these conditions.
Remember: with scarring alopecia, time is follicles. Every day of untreated inflammation is another day of potential permanent loss. Urgency isn’t overreaction. It’s appropriate medical care.
References
- Cicatricial Alopecia: Classification and Histopathology - Journal of the American Academy of Dermatology
- Frontal Fibrosing Alopecia: A Review - PubMed Central
- Scarring Alopecia: Diagnosis and Treatment - American Academy of Dermatology
- Central Centrifugal Cicatricial Alopecia: Pathogenesis and Treatment - PubMed
- Lichen Planopilaris: Clinical and Pathologic Study - Journal of the American Academy of Dermatology