You’ve been treating what you thought was stubborn dandruff for months. The flaking won’t quit. Your scalp itches. And now you’re noticing small patches where your hair seems thinner, almost broken off at the roots. Your dermatologist takes one look and says: “That’s not dandruff. It’s tinea capitis.”
Most people associate scalp ringworm with children. And they’re right to, because about 90% of cases occur in kids under 12. But adult cases exist, and they’re frequently misdiagnosed because doctors don’t expect to see them. A 2017 study in the Journal of the American Academy of Dermatology found that adult tinea capitis cases often go unrecognized for months, with patients receiving incorrect treatments for seborrheic dermatitis or psoriasis before the correct diagnosis is made.
Here’s the thing: if you’re an adult with a scaly, itchy scalp that isn’t responding to dandruff shampoo, you need to consider fungal infection. Because unlike dandruff or dermatitis, tinea capitis requires oral medication. Topical treatments can’t reach the fungus living inside your hair follicles. And the longer it goes untreated, the more permanent the hair loss becomes.
What Tinea Capitis Actually Is
Tinea capitis is a dermatophyte fungal infection of the scalp and hair shafts. The fungi responsible (usually Trichophyton tonsurans in the Gulf region and North America, or Microsporum canis in other areas) invade the hair follicle itself, growing down into the root structure. This is why the infection causes hair breakage and loss, something you don’t see with surface-level conditions like seborrheic dermatitis.
The fungus feeds on keratin, the protein that makes up your hair and the outer layer of your skin. As it grows, it weakens the hair shaft, causing it to break off near the scalp surface. You’re left with short, stubby hairs or even “black dots” where the broken shaft sits just below the skin. In severe cases, the immune response to the fungus creates a boggy, inflamed mass called a kerion, which can lead to permanent scarring and hair loss if not treated quickly.
Adults get tinea capitis less often than children, but when they do, it’s usually because of close contact with an infected child, occupational exposure (healthcare workers, teachers, daycare staff), immunosuppression, or living in crowded conditions. Pet contact matters too. Cats and dogs can carry Microsporum canis and transmit it to humans through direct contact or contaminated grooming tools.
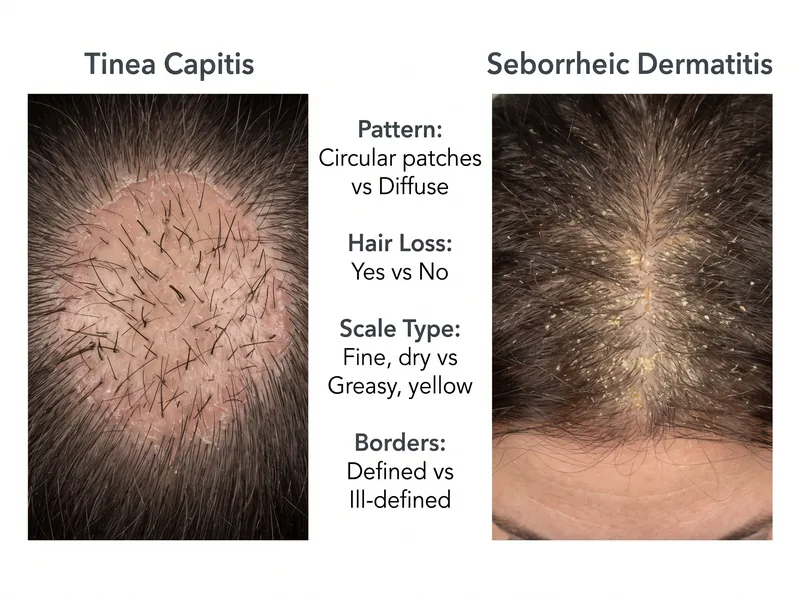 Tinea capitis shows circular patches with broken hairs and defined borders, while seborrheic dermatitis presents with diffuse yellow-white flaking without hair loss.
Tinea capitis shows circular patches with broken hairs and defined borders, while seborrheic dermatitis presents with diffuse yellow-white flaking without hair loss.
Why It Gets Misdiagnosed So Often
The clinical presentation of tinea capitis in adults overlaps significantly with other common scalp conditions. You see scaling? Could be dandruff. Redness and itching? Maybe eczema. Circular patches? Possibly alopecia areata. The problem is that doctors often default to the most common diagnosis (seborrheic dermatitis) without considering fungal infection, especially in adults where it’s rare.
The American Academy of Dermatology notes that adult cases are frequently mistaken for bacterial folliculitis, psoriasis, or even early scarring alopecia. The key differentiator is the pattern of hair loss. Tinea capitis causes patchy hair loss with broken hairs at varying lengths within the patch. The borders of the patches are often slightly raised and scaly. Seborrheic dermatitis, by contrast, causes diffuse flaking without focal hair loss.
Another confounding factor: some adults with tinea capitis don’t show the classic “ringworm” appearance. Instead, they present with diffuse scaling and minimal hair loss, which looks identical to dandruff. This “gray patch” variant is more common with T. tonsurans infections. Without a fungal culture or KOH prep test, it’s impossible to distinguish visually.
And here’s what makes it worse. Many adults self-treat with over-the-counter antifungal shampoos (ketoconazole, selenium sulfide) and see temporary improvement in the scaling. This gives false reassurance that it’s just dandruff, when in reality the topical antifungal is only suppressing surface symptoms without eradicating the infection in the follicle. The fungus persists, and the hair loss continues.
The Diagnostic Tests That Confirm It
If your doctor suspects tinea capitis, they’ll perform one or more of these tests. The quickest is a KOH (potassium hydroxide) preparation. They’ll pluck a few hairs from the affected area, place them on a slide with KOH solution, and examine them under a microscope. The KOH dissolves the keratin debris, making fungal hyphae and spores visible. If they see fungal elements inside or around the hair shaft, the diagnosis is confirmed.
But KOH prep has limitations. It requires skill to perform and interpret, and the sensitivity is only about 60-80%. A negative KOH doesn’t rule out tinea capitis. That’s why the gold standard is fungal culture. Your doctor will pluck hairs (with roots intact) and scales from the affected area and send them to a lab for culture. The culture identifies the specific organism and tests its susceptibility to antifungal drugs. Results take 2-4 weeks, which is frustratingly slow, but it’s the most definitive test.
Some dermatology practices use a Wood’s lamp (ultraviolet light) to screen for certain types of tinea capitis. Microsporum species fluoresce bright green under Wood’s lamp, making them easy to spot. But Trichophyton species (the most common cause in the Gulf and North America) don’t fluoresce. So a negative Wood’s lamp doesn’t rule anything out.
In ambiguous cases, especially when scarring alopecia is in the differential diagnosis, your dermatologist might perform a scalp biopsy. The biopsy shows fungal invasion of the hair follicle on histopathology and rules out other causes of patchy hair loss like alopecia areata or lichen planopilaris.
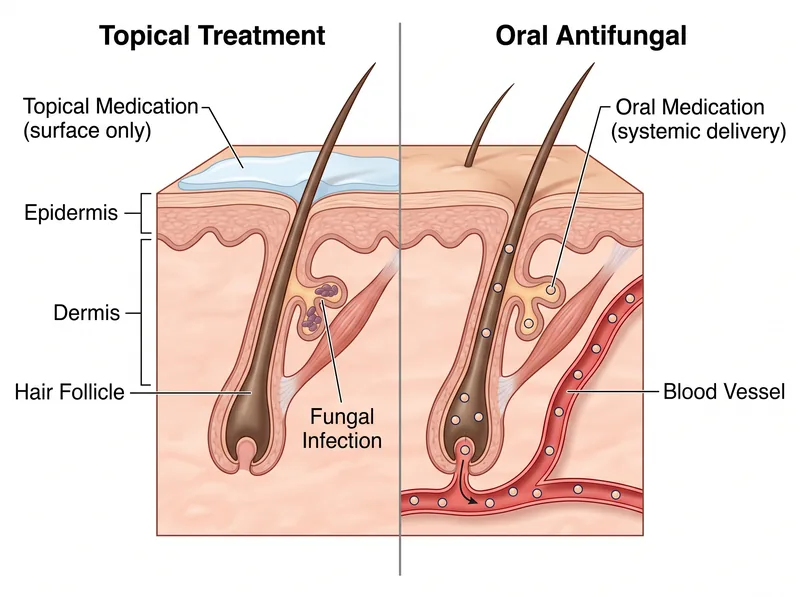 Oral antifungals reach the hair follicle through the bloodstream, while topical treatments can’t penetrate deep enough to eliminate the infection.
Oral antifungals reach the hair follicle through the bloodstream, while topical treatments can’t penetrate deep enough to eliminate the infection.
Why Topical Treatments Fail
This is the critical point that patients and even some primary care doctors miss. Tinea capitis requires oral antifungal medication because the infection lives inside the hair follicle, below the skin surface. Topical antifungals (shampoos, creams, lotions) can’t penetrate deep enough to reach the fungus.
Research published in the Journal of Fungi demonstrates that dermatophytes colonizing the hair shaft are protected by the hair cuticle and follicular epithelium. Topical agents applied to the scalp surface achieve minimal penetration into the follicle. They might reduce surface scaling and spore shedding (which helps prevent transmission), but they won’t cure the infection.
Oral antifungals work because they’re absorbed into the bloodstream and delivered to the hair follicle through the dermal blood supply. The medication concentrates in the growing hair shaft, creating a fungicidal environment that kills the dermatophyte. This is why cure rates with oral therapy (griseofulvin, terbinafine, itraconazole) are 80-95%, while topical monotherapy fails in nearly all cases.
That said, topical antifungals do have a role. They’re used as adjunctive therapy alongside oral medication to reduce spore shedding and prevent transmission to others. Your dermatologist will likely prescribe both an oral antifungal and a ketoconazole or selenium sulfide shampoo to use twice weekly. But the shampoo alone won’t cure you.
The Oral Antifungals That Actually Work
Griseofulvin has been the traditional first-line treatment for tinea capitis for decades. It’s fungistatic (stops fungal growth rather than killing directly) and requires a longer treatment course, usually 6-12 weeks. The standard adult dose is 500-1000mg daily, taken with fatty food to enhance absorption. Griseofulvin is generally well-tolerated, but it can cause headaches, GI upset, and photosensitivity. It also interacts with oral contraceptives, reducing their effectiveness.
Terbinafine is increasingly preferred, especially for Trichophyton infections. It’s fungicidal (directly kills the fungus) and has a shorter treatment duration, typically 4-6 weeks. The adult dose is 250mg daily. A 2018 meta-analysis in JAMA Dermatology found that terbinafine had higher cure rates and fewer side effects than griseofulvin for T. tonsurans infections. The main side effects are GI upset and, rarely, liver enzyme improvion or taste disturbance.
Itraconazole is a third option, used when the other two fail or aren’t tolerated. It’s dosed at 200mg daily for 4-6 weeks. Itraconazole has more drug interactions than the others and requires monitoring of liver function, but it’s effective against a broad range of dermatophytes.
Your dermatologist will choose the medication based on the organism identified on culture (if available), your medical history, and potential drug interactions. They’ll also monitor you during treatment with periodic lab tests to check liver function, especially if you’re on terbinafine or itraconazole for more than a few weeks.
Environmental Decontamination and Preventing Reinfection
Treating your scalp infection is only half the battle. You also need to decontaminate your environment to prevent reinfection or transmission to family members. Fungal spores can survive on combs, brushes, hats, pillowcases, and upholstery for months.
Start with personal items. Throw away or disinfect all combs, brushes, hair ties, and headbands. Soak them in a 1:10 bleach solution for 30 minutes, then rinse thoroughly. Replace your pillowcases and wash all bedding in hot water (at least 60°C) with detergent. Do the same with hats, scarves, and hooded clothing. If you’ve been to a barber or salon recently, notify them so they can disinfect their tools.
If you have pets, take them to a vet for evaluation. Dogs and cats can be asymptomatic carriers of Microsporum canis. The vet can perform a fungal culture or Wood’s lamp exam. If your pet is infected, they’ll need antifungal treatment too (usually oral itraconazole plus topical lime sulfur dips).
During treatment, avoid sharing personal items with others. Don’t let anyone else use your comb, towel, or pillow. If you’re living in the Gulf region where hard water is common, consider using a chelating shampoo like Regrowth+ to remove mineral buildup that can trap fungal spores on the scalp surface, making antifungal treatment less effective. Hard water deposits create a physical barrier that reduces the penetration of topical adjunctive treatments.
When Permanent Hair Loss Happens
Most cases of tinea capitis, if treated promptly, result in complete hair regrowth within 6-12 months after the infection clears. But delayed treatment or severe inflammatory response can lead to permanent scarring alopecia.
The most concerning complication is a kerion, a boggy, pus-filled inflammatory mass that develops when the immune system mounts an aggressive response to the fungus. Kerions are painful, swollen, and can drain pus. If not treated quickly with oral antifungals and sometimes oral corticosteroids to reduce inflammation, the intense immune reaction destroys the hair follicles permanently. You’re left with smooth, scarred patches where hair will never grow again.
Even without kerion formation, chronic untreated tinea capitis can cause follicular destruction through persistent inflammation. Hair regrowth timelines vary, but if you’ve had symptoms for more than 6 months before starting treatment, the likelihood of complete recovery decreases. This is why early diagnosis matters so much.
If you’re noticing persistent bald patches after completing antifungal treatment, see your dermatologist for a follow-up scalp exam and possibly a biopsy. They’ll assess whether the follicles are permanently damaged or if there’s residual inflammation that needs additional treatment.
What to Do If You Suspect Tinea Capitis
Don’t self-diagnose and don’t waste time with over-the-counter antifungal shampoos as monotherapy. If you have patchy hair loss with scaling, broken hairs, or persistent itching that hasn’t responded to dandruff treatment, see a dermatologist. Tell them you’re concerned about tinea capitis and ask for a KOH prep or fungal culture.
Be prepared for the possibility that your first doctor visit might not yield a diagnosis. If your primary care doctor dismisses your concern or prescribes only topical steroids or antifungal shampoo without testing, push for a referral to dermatology. Adult tinea capitis is uncommon enough that many general practitioners don’t consider it in their differential diagnosis.
Once you start oral antifungal treatment, be patient. You won’t see immediate improvement. It takes 2-4 weeks for the medication to reach therapeutic levels in the hair follicle, and you won’t see new hair growth until the infected hairs shed and new, healthy hairs grow in. The full treatment course is 4-12 weeks depending on the medication and organism. Don’t stop early, even if your symptoms improve, because incomplete treatment leads to relapse.
And if you’re experiencing hair loss from other causes in addition to the fungal infection, address those factors too. Nutritional deficiencies, hormonal imbalances, and chronic stress can all slow your recovery. Your dermatologist can order complete blood work to identify and correct these issues alongside antifungal treatment.
References
- Tinea Capitis in Adults: An Update on Diagnosis and Treatment - Journal of the American Academy of Dermatology
- Scalp Ringworm: Signs and Symptoms - American Academy of Dermatology
- Dermatophyte Infections and Antifungal Resistance Mechanisms - Journal of Fungi
- Comparative Efficacy of Antifungal Agents for Tinea Capitis: A Meta-analysis - JAMA Dermatology