This article contains affiliate links. See our affiliate disclosure for details.
You’re losing more hair than you’re growing. The drain catches more each day. Your hairline creeps back. The crown thins. And the internet offers a thousand solutions, most of them useless.
Here’s what’s actually happening: male pattern hair loss (androgenetic alopecia) affects 50% of men by age 50. It’s not about stress or your shampoo or wearing hats. It’s about genetics and hormones, specifically how your hair follicles respond to dihydrotestosterone (DHT). The follicles miniaturize. The growth phase shortens. Eventually, they stop producing visible hair entirely.
But here’s the part nobody tells you upfront: the treatments that actually work have been the same for decades. The FDA has approved exactly two medications for male pattern hair loss, and everything else is either complementary or experimental. This isn’t because science has stalled. It’s because these two treatments work well enough that pharmaceutical companies struggle to beat them in clinical trials.
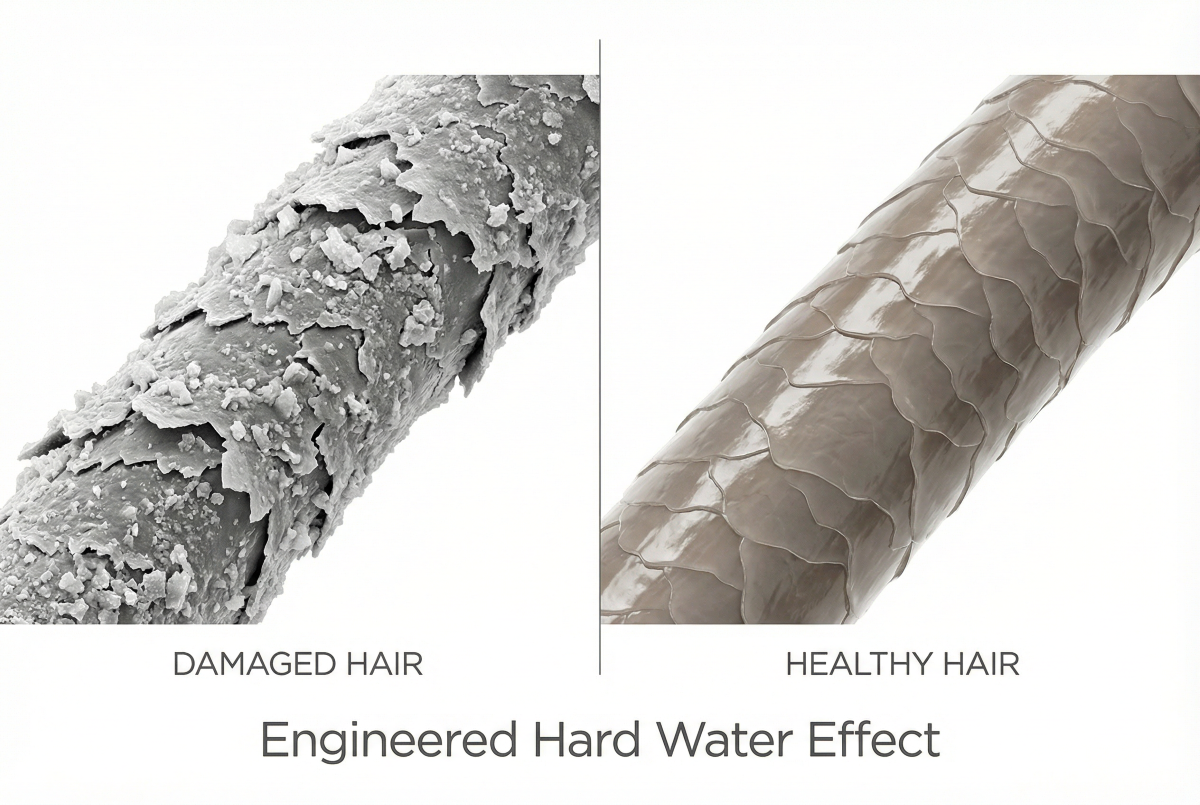
The challenge for men in the Gulf region is compounded by environmental factors. Hard water with high mineral content can accelerate the appearance of thinning by coating hair shafts and irritating the scalp, making existing hair loss more visible. That’s why addressing environmental factors alongside medical treatment produces better visible results than medication alone.
This guide covers what actually works, what the evidence shows, and how to build a treatment protocol that addresses both the hormonal cause and the environmental factors making it worse.
Minoxidil: The Blood Flow Solution
Minoxidil (brand name Rogaine) was the first FDA-approved hair loss treatment, discovered accidentally when doctors noticed hair growth as a side effect in blood pressure patients. It’s been studied extensively for over 30 years. The evidence is clear.
A meta-analysis of randomized controlled trials found that 5% minoxidil solution produced visible hair regrowth in 60% of men after 48 weeks of consistent use. That’s not marketing hype. That’s peer-reviewed clinical data.
How it works: Minoxidil is a vasodilator. It widens blood vessels around hair follicles, increasing nutrient and oxygen delivery. This extends the anagen (growth) phase of the hair cycle and appears to stimulate follicles from telogen (resting) back into active growth. The exact mechanism isn’t fully understood, but the results are reproducible.
Application matters. You need direct scalp contact twice daily. The foam version is less messy than liquid but both work equally well. Most men see initial shedding in weeks 2-4 (this is normal and temporary as weak hairs are replaced), then stabilization around month 3, and visible regrowth by month 6.
The catch: you can’t stop. Minoxidil doesn’t fix the underlying hormonal issue. It supports follicles while you use it. Stop using it, and within 3-4 months, you’ll return to baseline. This isn’t dependence. It’s just how the treatment works.
Side effects are minimal for most men. Scalp irritation occurs in about 5% of users. Facial hair growth can happen if solution drips onto the face (easily prevented with careful application). Serious cardiovascular effects are extremely rare at topical doses.
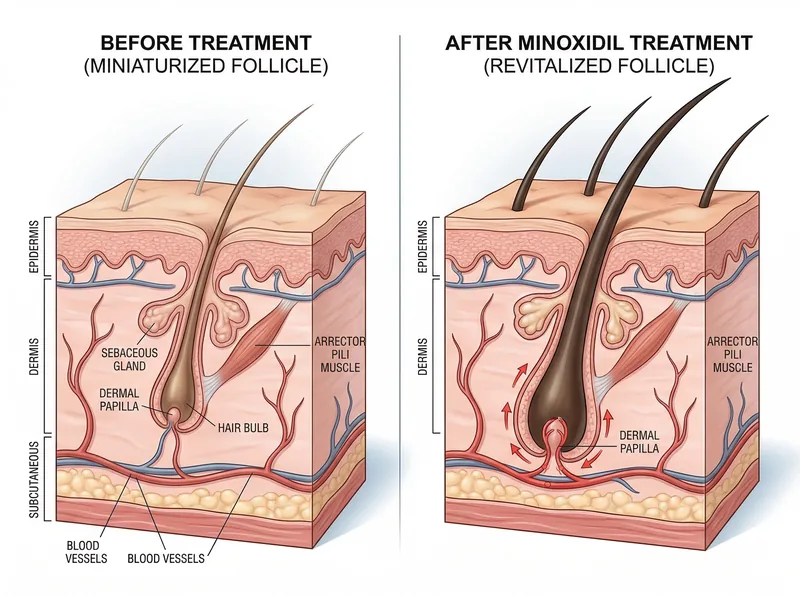 Minoxidil extends the growth phase of hair follicles by increasing blood flow and stimulating cellular activity in the dermal papilla.
Minoxidil extends the growth phase of hair follicles by increasing blood flow and stimulating cellular activity in the dermal papilla.
Finasteride: Blocking DHT at the Source
Finasteride (brand name Propecia) is the second FDA-approved treatment and the only one that addresses the hormonal cause of male pattern baldness. It’s a 5-alpha reductase inhibitor, meaning it blocks the enzyme that converts testosterone into DHT.
DHT is the villain in this story. It binds to androgen receptors in genetically susceptible hair follicles, triggering a miniaturization process. The follicles shrink. The hair shaft becomes thinner. The growth phase shortens. Eventually, the follicle produces only vellus hair (the fine, barely visible kind).
The landmark 5-year finasteride study showed that 90% of men maintained or increased their hair count compared to baseline. That’s remarkable durability for a hair loss treatment. The 1mg daily dose reduced scalp DHT levels by approximately 60%, which is enough to halt progression in most men.
Results timeline: Shedding may occur in the first 3 months (same as minoxidil, it’s a good sign). Stabilization happens around month 6. Visible regrowth, if it occurs, becomes apparent between months 6-12. Peak results typically appear at 2 years.
The side effect conversation: Sexual side effects (decreased libido, erectile dysfunction) occur in 1.8% of men taking finasteride versus 1.3% taking placebo in clinical trials. That’s a real but small increase. For most men, these effects resolve after discontinuation. A tiny subset reports persistent symptoms, though causation remains debated in the medical literature.
Here’s what matters: you need to weigh the proven benefits (halting hair loss in 90% of men) against the small risk of side effects. For many men, that’s an acceptable trade-off. For others, it’s not. There’s no wrong answer, but you need accurate data to decide.
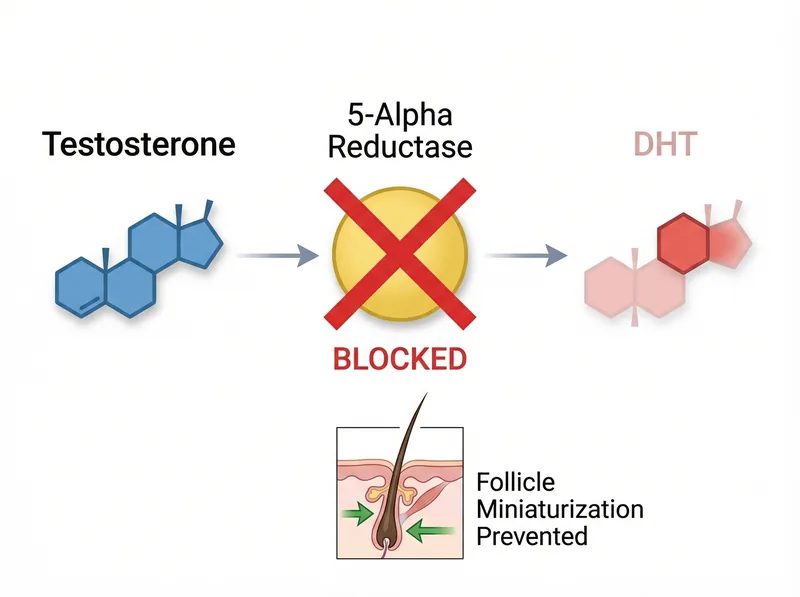 Finasteride blocks the enzyme 5-alpha reductase, preventing testosterone conversion to DHT, the hormone responsible for miniaturizing hair follicles.
Finasteride blocks the enzyme 5-alpha reductase, preventing testosterone conversion to DHT, the hormone responsible for miniaturizing hair follicles.
Low-Level Laser Therapy: The Dark Horse
Low-level laser therapy (LLLT) sounds like pseudoscience until you read the studies. FDA-cleared devices using red light wavelengths (650-670nm) have shown statistically significant improvements in hair count and thickness in randomized controlled trials.
The proposed mechanism: photobiomodulation. Red light at specific wavelengths penetrates the scalp and appears to stimulate cellular metabolism in hair follicles, increasing ATP production and promoting cell proliferation. It’s not as well-understood as minoxidil or finasteride, but the clinical outcomes are consistent.
Devices include laser caps, helmets, and combs. Treatment requires 20-30 minutes several times per week. Results appear slower than medication, typically 4-6 months for visible changes. The advantage is zero systemic side effects since it’s non-invasive and doesn’t involve drugs.
The downside is cost. Quality LLLT devices range from $200-$3000. That’s significantly more expensive than generic minoxidil and finasteride. For men who can’t or won’t use medication, LLLT offers an evidence-based alternative. For others, it works best as an adjunct to medical treatment.
Microneedling: The Synergistic Enhancer
Microneedling involves using a dermaroller or dermapen with tiny needles (typically 0.5-1.5mm) to create controlled micro-injuries in the scalp. This triggers wound healing responses that appear to enhance hair growth, particularly when combined with minoxidil.
A study comparing microneedling plus minoxidil versus minoxidil alone found that the combination group showed significantly greater hair count increases (91.4 vs 22.2 hairs per cm²). That’s a dramatic difference for a relatively simple intervention.
The mechanism likely involves multiple pathways: increased growth factor release, enhanced absorption of topical treatments, stimulation of stem cells in the hair bulge region, and improved blood flow from the healing response. It’s not magic. It’s controlled injury triggering repair.
Protocol matters. Most studies use 1.5mm needles once every 1-2 weeks, avoiding minoxidil application on the same day (to prevent systemic absorption through open channels). Home dermarollers work but require proper sterilization. Professional dermapen treatments offer more precision and depth control.
This isn’t a standalone treatment. Microneedling works best as an enhancer for minoxidil or as part of a complete protocol. Used alone, results are modest.
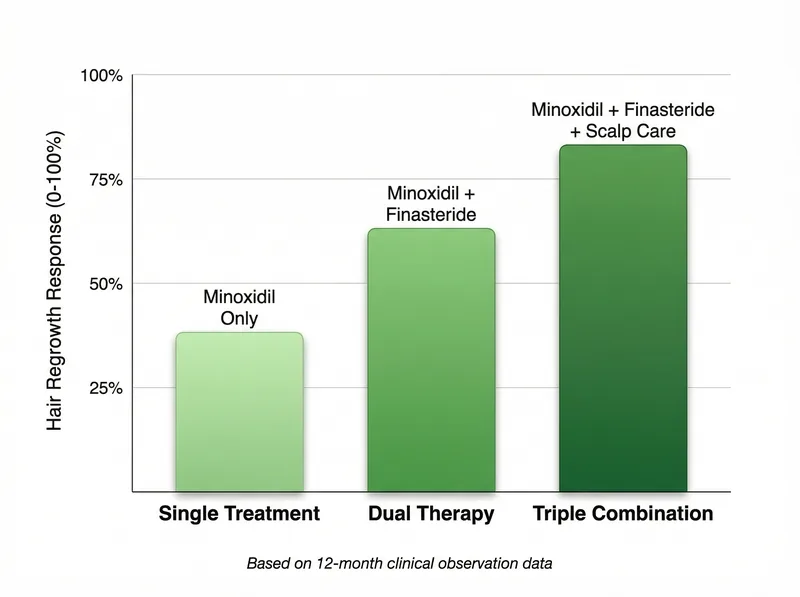 Combination therapy (minoxidil + finasteride + scalp improvation) shows significantly better outcomes than single-treatment approaches in clinical studies.
Combination therapy (minoxidil + finasteride + scalp improvation) shows significantly better outcomes than single-treatment approaches in clinical studies.
The Gulf Factor: Why Environment Matters
Medical treatments address the hormonal cause of hair loss. But in the Gulf region, environmental factors accelerate the visible progression. Hard water doesn’t cause androgenetic alopecia, but it makes existing hair loss look worse faster.
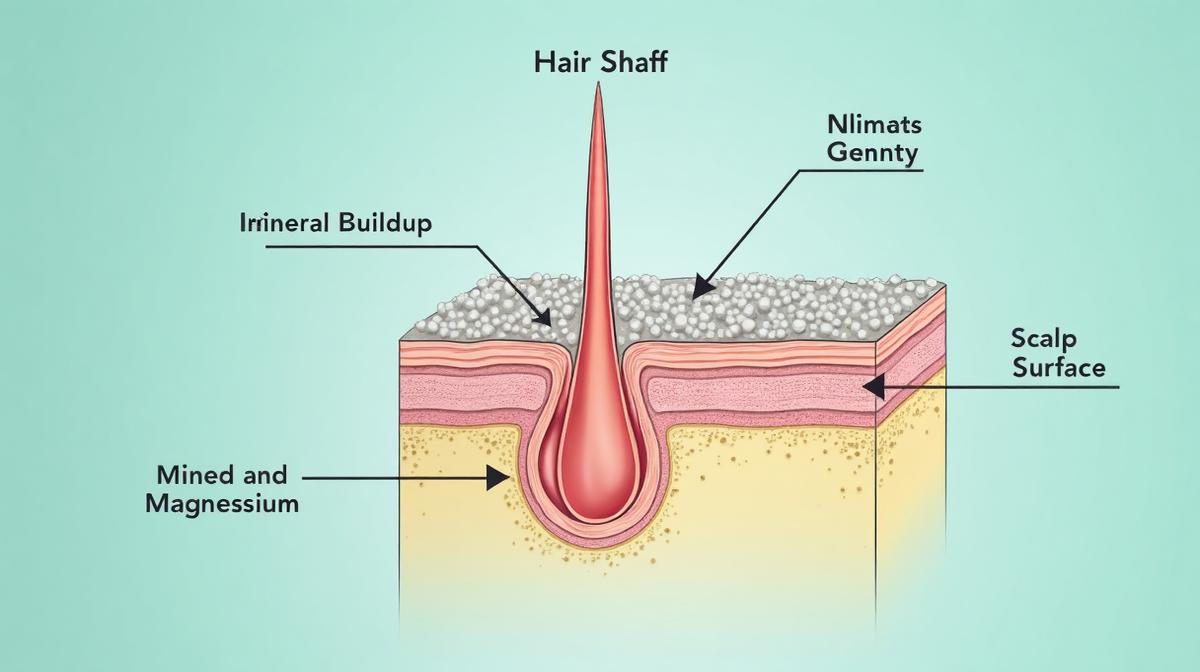
Here’s why: Gulf water contains 200-400 ppm of dissolved minerals (calcium, magnesium, silica). These minerals bind to hair proteins and scalp tissue. The result is a coating that makes hair shafts appear thinner, creates scalp inflammation that may accelerate follicle miniaturization, and reduces the effectiveness of topical treatments by creating a barrier.
This is where chelating shampoos become relevant. A chelating shampoo like Regrowth+ uses ingredients like EDTA and citric acid to dissolve mineral deposits without stripping natural oils. This isn’t about hair growth. It’s about creating optimal conditions for medical treatments to work and preventing environmental factors from compounding genetic hair loss.
The protocol: chelate once weekly to remove buildup, use minoxidil on a clean scalp for better absorption, continue finasteride for DHT suppression, and consider microneedling monthly to enhance treatment penetration. Address both the cause and the environment.
What Doesn’t Work: Clearing the Noise
Let’s eliminate the clutter. Biotin supplements don’t treat male pattern baldness unless you have a biotin deficiency (extremely rare). The American Academy of Dermatology states there’s no evidence biotin promotes hair growth in people with adequate nutrition.
Caffeine shampoos show weak evidence in isolated studies but nothing approaching the efficacy of minoxidil. Saw palmetto (a natural DHT blocker) has theoretical appeal but inconsistent clinical results. Ketoconazole shampoo has mild anti-androgenic effects but works better as an adjunct than a standalone treatment.
Hair vitamins are profitable marketing, not medicine. Unless you have a diagnosed deficiency (iron, vitamin D, zinc), supplementation won’t address androgenetic alopecia. The exception: vitamin D deficiency is common in the Gulf despite abundant sunlight (due to indoor lifestyles and sun avoidance), and correcting deficiency may improve overall hair health.
Laser combs sold through infomercials often lack the power output and wavelength precision of FDA-cleared devices. Not all red light is therapeutic. Platelet-rich plasma (PRP) shows promise in studies but remains expensive, requires multiple sessions, and has variable results depending on preparation protocols.
Building Your Treatment Protocol
Start with the foundation: minoxidil 5% twice daily for all men, finasteride 1mg daily for those willing to accept the small side effect risk. This combination halts progression in most men and produces regrowth in many. Everything else is supplementary.
Add environmental improvation for the Gulf context: weekly chelating to remove mineral buildup, quality water filtration if possible, protection from harsh sun and humidity. These don’t treat hair loss directly but prevent environmental factors from sabotaging your medical treatment.
Consider enhancement: microneedling once every 1-2 weeks to boost minoxidil absorption, LLLT 3 times weekly if budget allows, ketoconazole shampoo twice weekly for its mild anti-androgenic effects. These are evidence-based additions, not replacements for core treatment.
Timeline expectations: 3 months for stabilization, 6-12 months for visible regrowth, 2 years for peak results. Hair growth is slow. Follicles cycle through phases that take months. Anyone promising faster results is lying.
The reality check: not everyone responds equally. Genetics determines how sensitive your follicles are to treatment. Younger men with recent hair loss respond better than older men with long-standing baldness. Vertex (crown) loss responds better than frontal recession. Set realistic expectations based on evidence, not marketing.
References
- Topical minoxidil in the treatment of androgenetic alopecia - PubMed
- Finasteride in the treatment of men with androgenetic alopecia - PubMed
- The effectiveness of treatments for androgenetic alopecia: A systematic review - PubMed
- Low-level laser therapy for the treatment of androgenetic alopecia - PubMed
- Microneedling with dermaroller enhances minoxidil efficacy - PubMed