This article contains affiliate links. See our affiliate disclosure for details.
You’ve tried every anti-dandruff shampoo. The flakes keep coming back, thicker than before. Your scalp itches constantly, and when you scratch, you see silvery scales under your nails. Your dermatologist just said ‘psoriasis,’ and suddenly you’re wondering what that actually means for your hair.
Here’s what matters: scalp psoriasis isn’t dandruff. It’s not seborrheic dermatitis either, though they look similar enough to confuse even experienced clinicians at first glance. It’s an autoimmune condition where your skin cells multiply too quickly, creating those characteristic thick, silvery plaques that can extend beyond your hairline onto your forehead, neck, and ears.
About 50% of people with psoriasis develop scalp involvement at some point. For many, the scalp is the first place it appears. The good news? Modern treatments work remarkably well when you understand what you’re dealing with and stick with the protocol. This guide walks you through identification, triggers, and the treatment options that actually have evidence behind them.
How Scalp Psoriasis Differs from Other Scalp Conditions
The confusion is understandable. All three conditions, dandruff, seborrheic dermatitis, and scalp psoriasis, produce flaking. But the mechanisms and presentations are distinct once you know what to look for.
Scalp psoriasis creates thick, well-defined plaques with a silvery-white scale. The borders are sharp. When you lift the scale, you’ll often see pinpoint bleeding underneath (called the Auspitz sign). The plaques feel raised, almost like a layer of wax has been applied to your scalp. They commonly extend beyond the hairline, onto the forehead, behind the ears, down the nape of the neck. That extension is a key diagnostic clue.
Seborrheic dermatitis, by contrast, produces yellowish, greasy scales. The borders are less defined, more diffuse. It concentrates in areas with high sebum production, the crown, behind the ears, along the hairline, but doesn’t typically extend onto the face with the same sharp demarcation. The scales are softer, oilier to the touch.
Regular dandruff is the mildest form of seborrheic dermatitis, small, white, dry flakes without the inflammation or thick scale buildup. No raised plaques, no bleeding when scales are removed, minimal redness.
The underlying biology matters. Psoriasis is an autoimmune condition driven by T-cell activation and inflammatory cytokines that accelerate keratinocyte turnover. Your skin cells that normally take 28-30 days to mature and shed are completing the cycle in just 3-5 days. That’s why the scale accumulates so quickly and thickly.
Seborrheic dermatitis involves Malassezia yeast overgrowth and inflammatory response to its metabolic byproducts. Different mechanism, different treatment approach. Misdiagnosis leads to treatment failure because you’re targeting the wrong pathway.
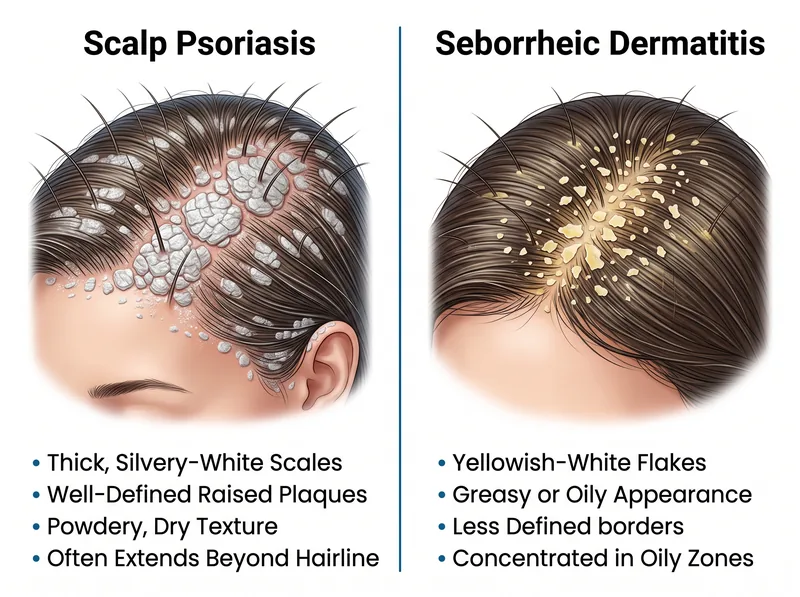 Key visual differences: psoriasis shows thicker silvery scales with defined borders, while seborrheic dermatitis presents with yellowish, greasy flakes and less distinct boundaries.
Key visual differences: psoriasis shows thicker silvery scales with defined borders, while seborrheic dermatitis presents with yellowish, greasy flakes and less distinct boundaries.
What Triggers Scalp Psoriasis Flares
Psoriasis isn’t caused by poor hygiene or contagion. It’s genetic susceptibility meeting environmental triggers. Understanding your personal trigger profile is half the battle.
Stress is the most commonly reported trigger. Not everyday annoyance, chronic, unmanaged stress that keeps cortisol improved and immune signaling dysregulated. Many patients report their first flare after a major life event: job loss, divorce, bereavement, relocation to the Gulf region.
Climate plays a significant role. Dry air worsens psoriasis for most people. The Gulf’s low humidity environment can be particularly challenging, though the intense sun exposure (when managed carefully) sometimes provides therapeutic benefit through natural UV exposure. But the dry indoor air from constant air conditioning? That’s a problem.
Infections, particularly strep throat, can trigger a specific type called guttate psoriasis that appears as small, drop-like lesions across the scalp and body. Even after the infection clears, the psoriasis can persist.
Certain medications are known triggers: beta-blockers, lithium, antimalarials, NSAIDs in some individuals. If your psoriasis appeared or worsened after starting a new medication, that’s a conversation to have with your prescribing physician. Don’t stop medications without medical guidance, but do raise the question.
Skin trauma, the Koebner phenomenon, means psoriasis can appear at sites of injury. Aggressive scratching, tight hairstyles causing traction, chemical treatments, even vigorous scalp massage can trigger new plaques along the trauma lines.
Alcohol and smoking both worsen psoriasis severity and reduce treatment effectiveness. The mechanisms involve immune dysregulation and increased inflammatory cytokine production. Cutting back makes a measurable difference in treatment response.
 Understanding your personal trigger profile helps you develop an effective prevention strategy alongside medical treatment.
Understanding your personal trigger profile helps you develop an effective prevention strategy alongside medical treatment.
Clinical Diagnosis: What Your Dermatologist Looks For
Visual inspection is usually sufficient for experienced dermatologists. They’re looking for the characteristic plaque morphology, scale type, distribution pattern, and extension beyond the hairline.
In ambiguous cases, dermoscopy (magnified examination) reveals diagnostic clues. Psoriasis shows regularly distributed dotted vessels, white scales, and a specific vascular pattern that differs from seborrheic dermatitis’s more irregular, curved vessels.
A scalp biopsy is rarely needed but definitively distinguishes psoriasis from other conditions. The histology shows characteristic features: thickened epidermis (acanthosis), elongated rete ridges, neutrophil collections in the stratum corneum (Munro microabscesses), dilated tortuous capillaries in the dermal papillae.
Your dermatologist will also ask about joint pain or stiffness. About 30% of people with psoriasis develop psoriatic arthritis, an inflammatory arthritis that requires different management. Morning stiffness, swollen fingers or toes, lower back pain, these warrant further evaluation.
Family history is relevant. If you have first-degree relatives with psoriasis, your risk increases significantly. The condition has strong genetic components involving multiple susceptibility loci, particularly HLA-Cw6.
Blood tests aren’t diagnostic for psoriasis itself, but your doctor might order them to rule out other conditions or establish baselines before starting systemic treatments. A complete metabolic panel, liver function, and lipid profile are standard if biologics or systemic medications are being considered.
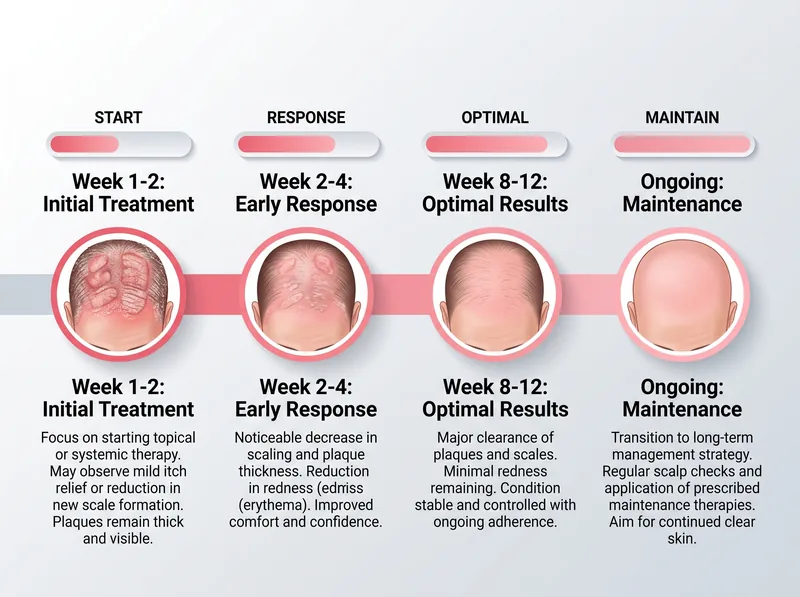 Most patients see initial improvement within 2-4 weeks of consistent treatment, with optimal results typically appearing after 8-12 weeks of adherence.
Most patients see initial improvement within 2-4 weeks of consistent treatment, with optimal results typically appearing after 8-12 weeks of adherence.
Treatment Options: From Topical to Systemic
Treatment selection depends on severity, extent of involvement, treatment history, and impact on quality of life. Most scalp psoriasis starts with topical therapy, escalating only if needed.
Coal tar shampoos remain a cornerstone treatment despite their old-fashioned reputation. Coal tar has anti-inflammatory, antiproliferative, and antipruritic properties. Concentrations typically range from 0.5% to 5%. The smell is distinctive (some say unpleasant), and it can temporarily darken light-colored hair, but efficacy is well-documented. Use it 2-3 times weekly, leaving it on the scalp for 5-10 minutes before rinsing.
Salicylic acid is a keratolytic, it breaks down the thick scale so other medications can penetrate. Concentrations of 2-3% in shampoo formulations work well. It’s often combined with coal tar for synergistic effect. Salicylic acid alone won’t control the inflammation, but it’s essential for descaling thick plaques.
For the Gulf’s hard water environment, starting with a chelating shampoo like Regrowth+ before applying medicated treatments can improve their effectiveness by removing mineral buildup that blocks active ingredient penetration.
Topical corticosteroids are the most prescribed treatment for scalp psoriasis. High-potency options like clobetasol propionate 0.05% solution or foam are used for initial control, then tapered to mid-potency maintenance. Apply to affected areas once or twice daily. Results appear within 2-4 weeks. The risk with long-term high-potency steroid use is skin atrophy and tachyphylaxis (reduced effectiveness over time), so most dermatologists recommend weekend-only maintenance after initial clearing.
Vitamin D analogs like calcipotriene slow skin cell turnover without the atrophy risk of steroids. They’re often combined with corticosteroids in single formulations (like Enstilar foam) for better efficacy than either agent alone. Calcipotriene can irritate facial skin, so be careful with application near the hairline.
Topical retinoids (tazarotene) normalize skin cell differentiation and reduce inflammation. They’re effective but can be irritating, particularly in the initial weeks. Often combined with corticosteroids to reduce irritation while maintaining efficacy.
Phototherapy, specifically narrowband UVB or excimer laser, is highly effective for scalp psoriasis but requires specialized equipment and multiple sessions per week. It’s typically reserved for cases not controlled by topicals or when patients want to avoid long-term medication use. The scalp’s hair coverage makes it technically challenging but not impossible.
Systemic medications are considered when scalp psoriasis is severe, extensive, or accompanied by psoriasis elsewhere on the body. Options include methotrexate, cyclosporine, acitretin, and apremilast. These require regular monitoring for side effects and aren’t first-line for scalp-only disease.
Biologics, injectable medications targeting specific immune pathways, have revolutionized severe psoriasis treatment. TNF-alpha inhibitors (adalimumab, etanercept), IL-17 inhibitors (secukinumab, ixekizumab), and IL-23 inhibitors (guselkumab, risankizumab) achieve clearance rates that were unthinkable 20 years ago. They’re expensive, require injection training, and carry infection risks, so they’re reserved for moderate-to-severe cases that haven’t responded to other treatments. But when appropriate, they’re remarkably effective.
Application Techniques That Actually Work
Even the best medication fails if you can’t get it onto the scalp through the hair. Technique matters as much as the prescription.
Part your hair in rows, about 1-2 cm apart, and apply medication directly to the scalp with the applicator tip or your fingertips. Don’t just pour it on top of your hair and hope it reaches the skin. You’re treating the scalp, not the hair shaft.
For thick plaques, descale first. Apply salicylic acid or a mineral oil-based descaling treatment, cover with a shower cap, leave it on for several hours or overnight, then shampoo. Once the thick scale is removed, your anti-inflammatory medications can actually reach the skin.
Timing matters. Most topical treatments work best when left on overnight. Apply before bed, sleep on an old pillowcase (some medications can stain), shampoo in the morning. If overnight isn’t feasible, aim for at least 4 hours of contact time.
Shampoo technique: wet hair thoroughly, apply medicated shampoo, massage gently into the scalp (not aggressive scrubbing that causes trauma), leave it on for the recommended time (usually 5-10 minutes), then rinse completely. Many people rinse too quickly and wonder why the shampoo doesn’t work.
Consistency beats intensity. Using your medication sporadically at high frequency when you remember won’t work as well as regular, sustained use at the prescribed frequency. Psoriasis treatment is a marathon, not a sprint.
When to Escalate Treatment
How do you know when your current treatment isn’t working well enough? Here’s the framework dermatologists use.
If you’ve used a topical regimen correctly and consistently for 8-12 weeks without significant improvement, that’s a signal to escalate. ‘Significant improvement’ means at least 50% reduction in plaque thickness, scale, and redness. If you’re still at 80% of baseline severity after three months of compliant treatment, the current approach isn’t sufficient.
Quality of life impact matters more than you might think. If your scalp psoriasis is causing significant psychological distress, social avoidance, or sleep changeion, even if the physical extent seems ‘mild’ by clinical measures, that warrants more aggressive treatment. The Dermatology Life Quality Index (DLQI) is a validated tool doctors use to quantify this impact.
Rapid spreading or sudden worsening despite treatment suggests either incorrect diagnosis, a new trigger (infection, medication, major stressor), or inadequate treatment potency. That’s a reason to revisit your dermatologist sooner rather than waiting for the next scheduled appointment.
Joint symptoms appearing alongside scalp psoriasis, morning stiffness, swollen joints, lower back pain, are red flags for psoriatic arthritis. This changes the treatment calculus entirely because you need systemic therapy to prevent joint damage, not just topical treatment for the skin.
Side effects from current treatment that are intolerable or dangerous (severe irritation, skin atrophy, systemic effects from absorbed medications) obviously require switching to alternative approaches.
References
- Pathogenesis and clinical features of psoriasis - National Center for Biotechnology Information
- Psoriatic arthritis: Symptoms and causes - Mayo Clinic
- Coal tar: an old therapy in contemporary dermatology practice - PubMed
- Quality of life in patients with psoriasis - National Center for Biotechnology Information
- Scalp psoriasis: clinical presentations and therapeutic management - American Academy of Dermatology