This article contains affiliate links. See our affiliate disclosure for details.
Your doctor ordered bloodwork. Everything came back ‘normal.’ But your hair’s still falling out in the shower, thinning at the crown, shedding on your pillow. Here’s the problem: standard lab panels aren’t designed to catch the nutritional deficiencies that trigger hair loss. They’re built to diagnose anemia, thyroid disease, and metabolic disorders, conditions where you’re symptomatic enough to need medical intervention. Hair thinning? That’s a ‘cosmetic concern’ in most clinical protocols.
But it’s not cosmetic when you’re watching your hairline recede or your part widen. And it’s definitely not normal when you’re in your twenties or thirties and losing hair faster than your parents did at fifty. The truth is, ferritin levels that trigger hair loss sit well above the clinical threshold for anemia. Thyroid dysfunction can wreck your hair growth cycle months before your TSH crosses into ‘abnormal’ territory. Vitamin D deficiency? Most labs flag it only when you’re at risk for bone disease, not when your follicles are starving for it.
This guide breaks down the specific blood tests that matter for hair loss, the reference ranges that actually correlate with healthy hair growth (not just ‘not sick’), and why you need to request these panels by name. Because if you don’t ask, you won’t get tested. And if you don’t get tested, you’re treating the symptom, shedding hair, without addressing the root cause.
Ferritin: The Hair Loss Marker Doctors Ignore
Ferritin measures your iron storage, not your circulating iron. And that distinction matters because hair follicles are metabolically expensive. They’re among the most rapidly dividing cells in your body, second only to bone marrow. When your body senses low iron stores, it triages. Essential functions, oxygen transport, red blood cell production, get priority. Hair growth? That’s expendable.
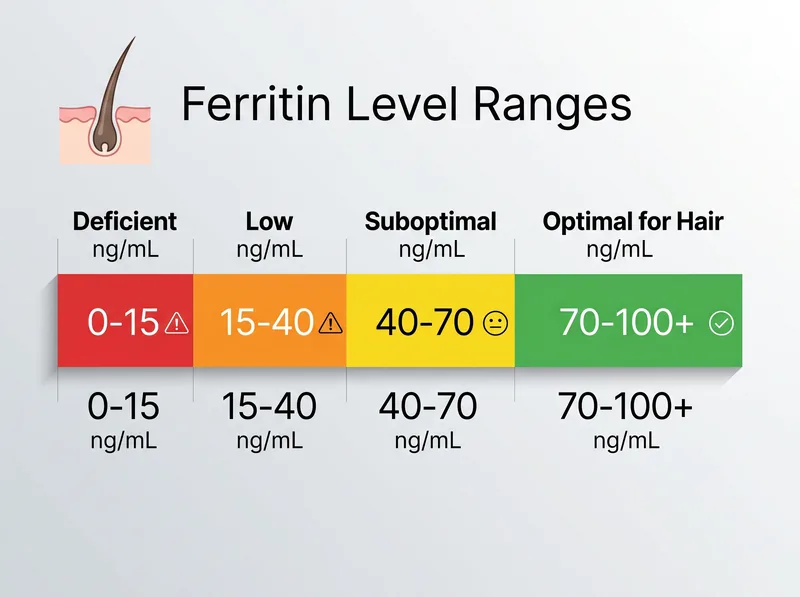
The clinical reference range for ferritin is typically 12-150 ng/mL for women and 12-300 ng/mL for men. But research published in the Journal of the American Academy of Dermatology found that ferritin levels below 40 ng/mL are associated with hair loss, even when hemoglobin remains normal. Some trichologists recommend maintaining ferritin above 70 ng/mL for optimal hair growth.
You can have a ferritin of 20 ng/mL, be told you’re ‘normal,’ and still experience diffuse hair shedding. The lab isn’t wrong, you’re not anemic. But your hair doesn’t care about clinical thresholds. It cares about having enough stored iron to fuel the anagen (growth) phase of the hair cycle.
Request a ferritin test specifically. Don’t settle for a CBC (complete blood count) alone, it measures hemoglobin and hematocrit, not storage iron. If your ferritin comes back below 40 ng/mL, supplementation under medical supervision is the standard intervention. But expect a slow response. It takes three to six months of consistent supplementation to rebuild iron stores and see visible improvement in hair density.
 Ferritin levels below 40 ng/mL can trigger hair thinning even when hemoglobin remains normal, a marker most standard panels ignore.
Ferritin levels below 40 ng/mL can trigger hair thinning even when hemoglobin remains normal, a marker most standard panels ignore.
Thyroid Panel: Why TSH Alone Isn’t Enough
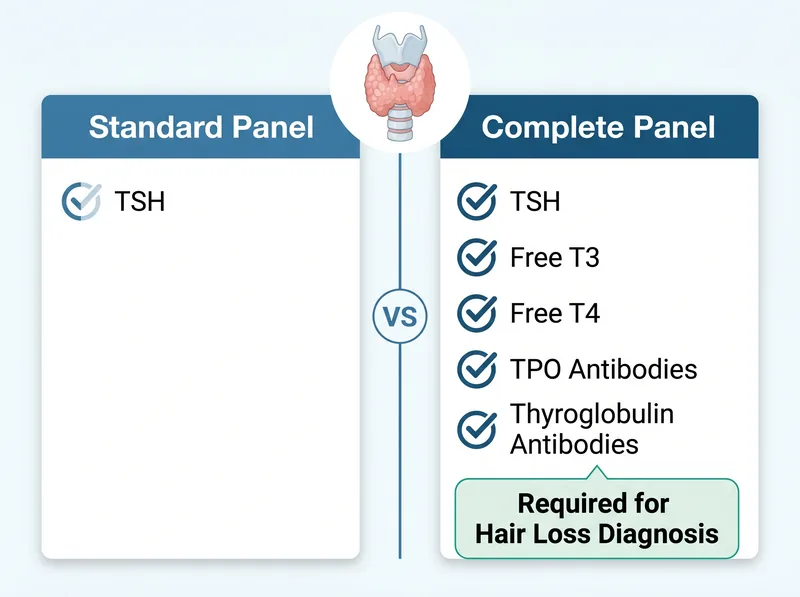
Most doctors order TSH (thyroid-stimulating hormone) as a screening test. If it’s normal, they assume your thyroid is fine. But TSH is a pituitary hormone, not a thyroid hormone. It tells you what your brain thinks your thyroid should be doing, not what your thyroid is actually producing. And that gap matters for hair loss.
You need a full thyroid panel: TSH, free T3, free T4, TPO antibodies, and thyroglobulin antibodies. Free T3 is the active form of thyroid hormone that binds to receptors in hair follicles. Studies show that subclinical hypothyroidism, where TSH is borderline high but free T3 and free T4 are low-normal, can trigger telogen effluvium, a diffuse shedding pattern that looks like generalized thinning.
Thyroid antibodies (TPO and thyroglobulin) detect autoimmune thyroid disease, which can cause hair loss even when thyroid hormone levels appear normal. Hashimoto’s thyroiditis, the most common cause of hypothyroidism in developed countries, often presents with hair thinning as an early symptom, sometimes years before TSH becomes clinically abnormal.
If your TSH is above 2.5 mIU/L and you’re experiencing hair loss, request the full panel. The reference range for TSH is typically 0.4-4.0 mIU/L, but functional medicine practitioners often target 1.0-2.0 mIU/L for optimal metabolic function. Free T3 should be in the upper half of the reference range, and free T4 should be mid-range or higher. Anything less, and your follicles aren’t getting the thyroid hormone they need to sustain the anagen phase.
 A standard TSH-only test misses subclinical thyroid dysfunction that can trigger diffuse hair shedding, request the full panel.
A standard TSH-only test misses subclinical thyroid dysfunction that can trigger diffuse hair shedding, request the full panel.
Vitamin D: The Deficiency Hiding in Plain Sight
Vitamin D isn’t just for bone health. It’s a steroid hormone that regulates over 200 genes, including those involved in hair follicle cycling. Research published in Skin Pharmacology and Physiology found that vitamin D receptors are present in hair follicles, and deficiency is linked to alopecia areata, telogen effluvium, and androgenetic alopecia.
The standard reference range for vitamin D (25-hydroxyvitamin D) is 30-100 ng/mL. But here’s the disconnect: levels below 30 ng/mL are flagged as ‘deficient’ for bone health, not hair health. Many dermatologists recommend maintaining vitamin D above 40-50 ng/mL for optimal hair growth, particularly in individuals with autoimmune or inflammatory scalp conditions.
Vitamin D deficiency is endemic in the Gulf region despite year-round sun exposure. Why? Cultural clothing that covers most of the skin, indoor lifestyles with air conditioning, and darker skin tones that require more UV exposure to synthesize vitamin D. If you’re experiencing unexplained hair thinning, request a 25-hydroxyvitamin D test. If it’s below 40 ng/mL, supplementation (typically 2,000-5,000 IU daily under medical guidance) can help, but it takes months to see results.
Zinc, DHEA-S, and Free Testosterone: The Supporting Cast
Zinc is a cofactor for over 300 enzymatic reactions, including those that regulate hair follicle stem cell activation. Zinc deficiency has been linked to telogen effluvium and alopecia areata, particularly in individuals with restrictive diets or malabsorption conditions. The serum zinc reference range is typically 60-120 mcg/dL, but optimal levels for hair health are thought to be above 80 mcg/dL.
DHEA-S (dehydroepiandrosterone sulfate) is an androgen precursor produced by the adrenal glands. In women, improved DHEA-S can signal PCOS (polycystic ovary syndrome), a hormonal condition that often presents with androgenetic alopecia, pattern hair loss driven by androgen sensitivity. If you’re a woman experiencing hair thinning along the central part or temples, request DHEA-S and free testosterone. Improved levels suggest a hormonal component that won’t respond to topical treatments alone.
Free testosterone (not total testosterone) measures the bioavailable hormone that can bind to androgen receptors in hair follicles. In men, low free testosterone can contribute to hair thinning, though the relationship is complex, DHT (a metabolite of testosterone) is the primary driver of androgenetic alopecia. In women, improved free testosterone often correlates with PCOS and androgenetic alopecia. The reference ranges vary by lab, but abnormal results warrant endocrinology referral.
These markers aren’t first-line tests for hair loss, but they’re worth requesting if ferritin, thyroid, and vitamin D come back normal and you’re still shedding. Zinc supplementation, for example, can help, but only if you’re actually deficient. Excess zinc interferes with copper absorption and can worsen hair loss, so don’t supplement without bloodwork confirmation.
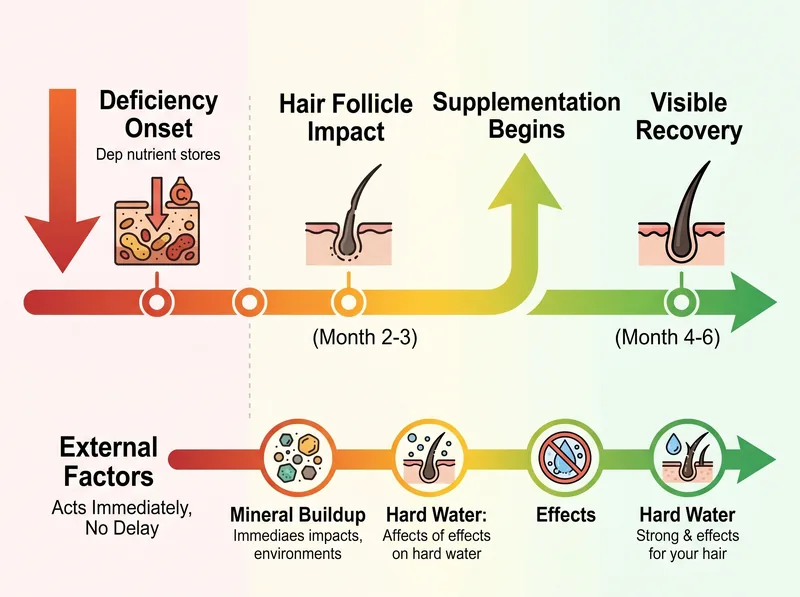 Internal nutritional deficiencies take 3-6 months to correct and show visible improvement, while external factors like mineral buildup act immediately.
Internal nutritional deficiencies take 3-6 months to correct and show visible improvement, while external factors like mineral buildup act immediately.
The Timeline Problem: Why Internal Fixes Take Months
Here’s the frustrating reality: even if you identify a deficiency and start supplementation, hair follicles don’t respond overnight. The hair growth cycle is slow. Each follicle spends 2-6 years in anagen (growth phase), a few weeks in catagen (transition), and 2-3 months in telogen (resting phase before shedding). When a nutritional deficiency changes the cycle, follicles shift prematurely into telogen. You don’t see the shedding immediately, it takes 2-3 months for those resting hairs to fall out.
Once you correct the deficiency, you have to wait for the follicle to re-enter anagen and grow a new hair. That process takes another 3-6 months. So from deficiency onset to visible recovery, you’re looking at six months minimum, often closer to a year. And that’s assuming the deficiency was the only problem.
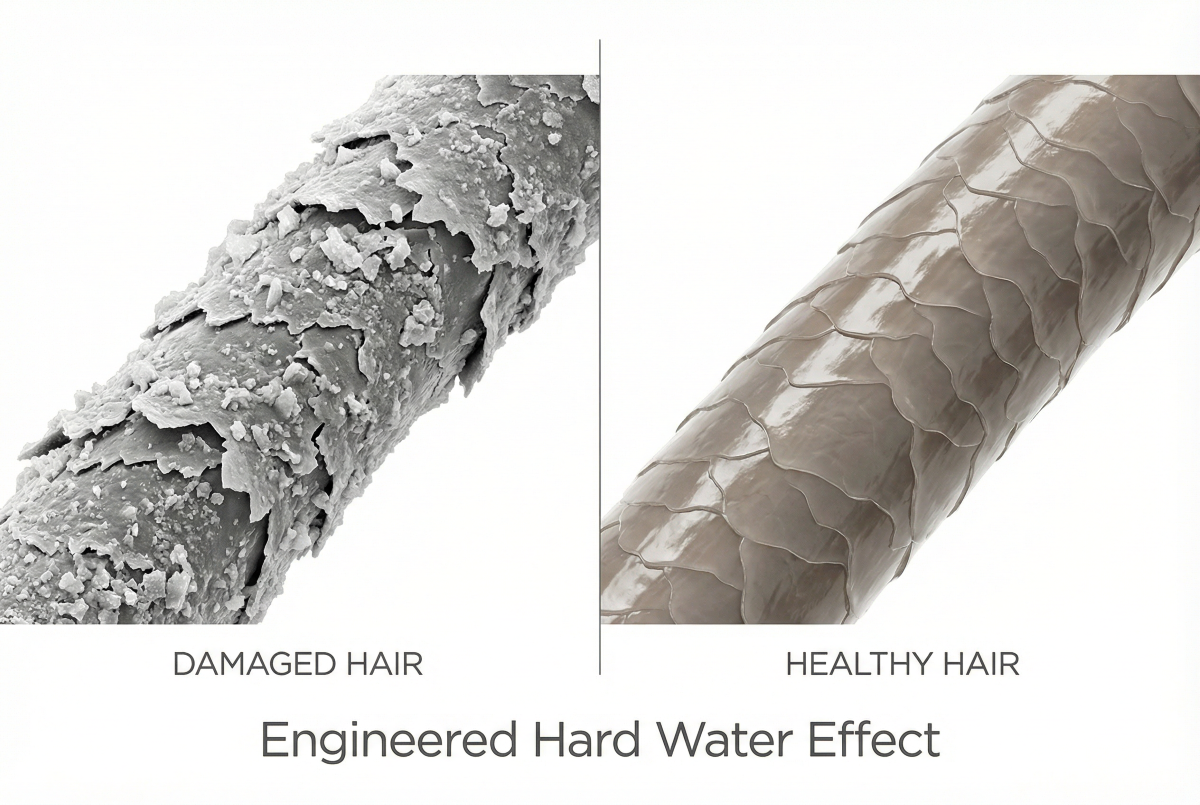
But here’s what most doctors don’t tell you: while you’re waiting for your ferritin to climb or your thyroid to stabilize, external factors are still attacking your hair. If you live in the Gulf, you’re showering in hard water with 400+ ppm of dissolved minerals. Those minerals, calcium, magnesium, silica, coat your hair shaft and scalp, creating a barrier that blocks moisture and clogs follicles. Hard water doesn’t cause deficiency-driven hair loss, but it compounds the damage by preventing your hair from recovering even after you fix the internal issue.
That’s why a chelating shampoo like Regrowth+ matters. It removes mineral buildup immediately, no waiting months for nutrient stores to rebuild. You address the internal deficiency with bloodwork and supplementation, and you address the external buildup with a chelating formula. Both levers matter. One without the other leaves you stuck in a cycle of slow progress and continued shedding.
How to Request the Right Tests (And What to Do If Your Doctor Refuses)
Most primary care doctors won’t order a complete hair loss panel unless you ask. And even if you ask, some will dismiss it as unnecessary if your CBC and basic metabolic panel are normal. Here’s how to navigate that conversation.
Be specific. Don’t say ‘I want bloodwork for hair loss.’ Say: ‘I’d like to request ferritin, a full thyroid panel including free T3 and free T4, 25-hydroxyvitamin D, and serum zinc.’ If you’re a woman with signs of hormonal imbalance (irregular periods, acne, hirsutism), add: ‘I’d also like DHEA-S and free testosterone to rule out PCOS.’
If your doctor refuses, ask why. If the answer is ‘those tests aren’t medically necessary,’ clarify that you’re willing to pay out of pocket if insurance won’t cover them. In many regions, you can order your own bloodwork through direct-to-consumer labs without a doctor’s order. It’s more expensive, but it bypasses the gatekeeper problem.
Once you have results, don’t accept ‘normal’ as the final answer. Ask for the actual numbers and compare them to the hair-specific thresholds discussed in this article. A ferritin of 25 ng/mL is ‘normal’ by lab standards but suboptimal for hair growth. A TSH of 3.5 mIU/L is ‘normal’ but borderline high if you’re experiencing symptoms. Advocate for yourself. If your doctor won’t engage, find a dermatologist or trichologist who specializes in hair loss. They’re more likely to understand the nuance.
References
- Serum ferritin and diffuse hair loss in women - Journal of the American Academy of Dermatology
- Thyroid hormones and hair follicle biology - PubMed Central
- The role of vitamin D in hair follicle cycling - Skin Pharmacology and Physiology
- Zinc status and hair loss: A systematic review - PubMed Central
- Nutritional factors and hair loss - American Academy of Dermatology