This article contains affiliate links. See our affiliate disclosure for details.
You’ve probably heard that DHT causes hair loss. But what does that actually mean? How does a hormone that’s essential for male development suddenly turn against your hair follicles in your twenties or thirties?
Here’s the thing: DHT doesn’t just damage follicles randomly. It follows a precise biochemical pathway that’s been mapped by decades of research. Understanding this mechanism explains why DHT-blocking treatments take so long to work, why some follicles are vulnerable while others aren’t, and why you can’t simply wash DHT away with shampoo.
But here’s what most dermatologists won’t tell you: while DHT is the internal driver of androgenetic alopecia, external factors like mineral buildup and harsh surfactants can accelerate the visible damage. Your follicles are fighting a war on two fronts, and most people only address one.
This guide breaks down the complete DHT mechanism, from the 5-alpha-reductase enzyme to follicle miniaturization, and explains how to manage both the internal hormonal axis and the external environmental factors that compound the problem.
The DHT Conversion Process: How Testosterone Becomes a Follicle Enemy
Dihydrotestosterone (DHT) isn’t produced directly by your body. It’s created when the enzyme 5-alpha-reductase converts testosterone into DHT in specific tissues, including hair follicles, prostate tissue, and sebaceous glands.
There are two types of 5-alpha-reductase. Type I is found primarily in sebaceous glands and skin. Type II is concentrated in hair follicles and the prostate. Research published in the Journal of Clinical Endocrinology & Metabolism shows that Type II is the dominant form in scalp follicles, which is why finasteride (which blocks Type II) is more effective for hair loss than treatments targeting Type I alone.
Once DHT is formed, it binds to androgen receptors inside follicle cells. This binding triggers a cascade of gene expression changes that gradually shrink the follicle over successive growth cycles. The process is slow, methodical, and cumulative.
Why does this matter? Because DHT isn’t floating around in your bloodstream waiting to attack your hair. It’s being produced locally, right inside the follicles themselves. You can have normal testosterone levels and still experience aggressive hair loss if your follicles have high 5-alpha-reductase activity or sensitive androgen receptors.
Genetics determine both factors. Some people inherit follicles with hyperactive 5-alpha-reductase. Others inherit androgen receptors that are unusually responsive to DHT. Both pathways lead to the same outcome: progressive miniaturization.
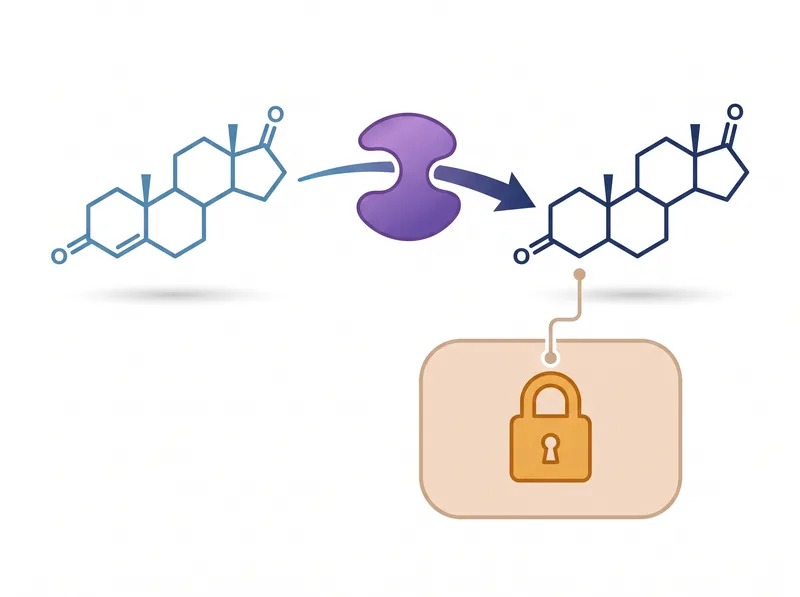 The 5-alpha-reductase enzyme converts testosterone into DHT, which then binds to androgen receptors in follicle cells and triggers the miniaturization cascade.
The 5-alpha-reductase enzyme converts testosterone into DHT, which then binds to androgen receptors in follicle cells and triggers the miniaturization cascade.
Follicle Miniaturization: The Gradual Shrinking Process
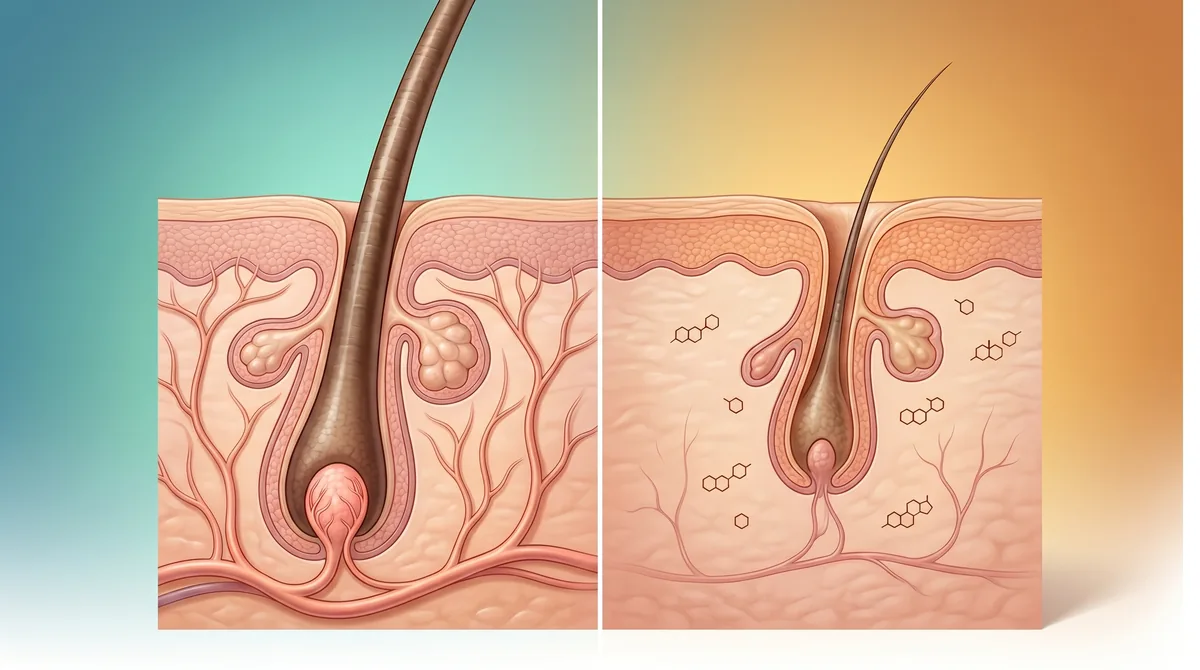
Miniaturization is the hallmark of androgenetic alopecia. It’s not sudden hair loss. It’s a slow transformation where terminal hairs (thick, pigmented, long-growing) gradually become vellus hairs (thin, colorless, short).
Each time a follicle completes a growth cycle, DHT shortens the anagen (growth) phase and extends the telogen (resting) phase. A study in Dermatologic Therapy documented that miniaturized follicles can have anagen phases as short as weeks instead of years.
With each cycle, the dermal papilla (the follicle’s command center) shrinks. Blood supply diminishes. The hair shaft becomes finer. The follicle retreats higher into the scalp. Eventually, it stops producing visible hair altogether and enters a dormant state.
But here’s the critical detail: miniaturized follicles aren’t dead. They’re dormant. This is why early intervention with DHT blockers can reverse some miniaturization. The follicle is still there, still capable of function, but suppressed by hormonal signaling.
The timeline varies wildly. Some men see aggressive miniaturization in their early twenties. Others maintain most of their hair into their fifties. Women typically experience diffuse thinning across the crown rather than the distinct recession pattern seen in men, though the underlying mechanism is identical.
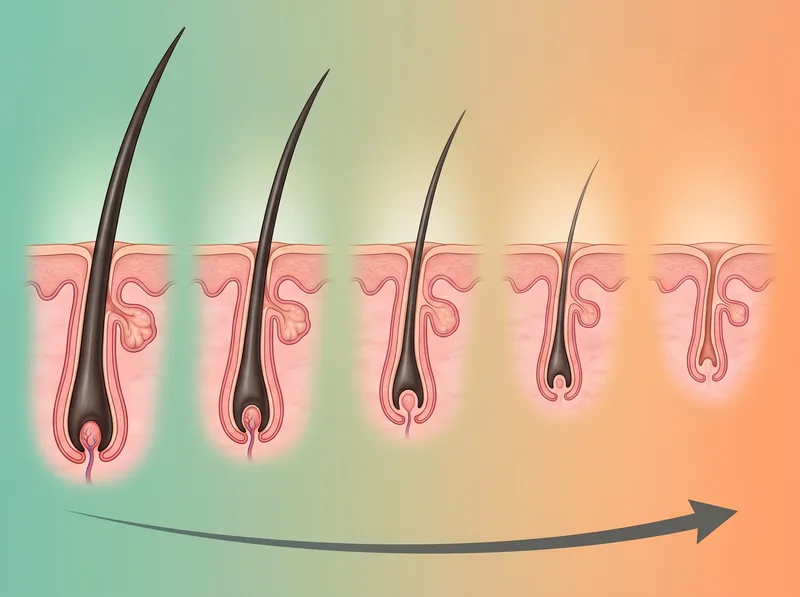 Follicle miniaturization happens gradually over years, with each growth cycle producing progressively thinner hair until the follicle becomes dormant.
Follicle miniaturization happens gradually over years, with each growth cycle producing progressively thinner hair until the follicle becomes dormant.
Why DHT Affects Some Follicles and Not Others
If DHT is everywhere in the scalp, why does hair loss follow predictable patterns? Why do men lose hair at the temples and crown but keep the sides and back? Why do women thin at the part but rarely go completely bald?
The answer lies in androgen receptor density and distribution. Research in the Journal of Investigative Dermatology found that follicles in the frontal and vertex scalp have significantly higher androgen receptor concentrations than follicles in the occipital (back) and temporal (side) regions.
This genetic programming explains the Norwood scale pattern in men and the Ludwig scale pattern in women. The follicles most vulnerable to DHT are clustered in specific zones, while the ‘safe donor zone’ at the back and sides remains largely unaffected even in advanced hair loss.
It also explains why hair transplants work. Follicles moved from the donor zone to the thinning areas retain their genetic resistance to DHT. They continue growing in their new location because their androgen receptor profile doesn’t change.
But genetics isn’t the only variable. Inflammation, oxidative stress, and poor blood flow can make follicles more vulnerable to DHT damage. This is where environmental factors enter the equation.
How DHT-Blocking Treatments Work (and Why They’re Slow)
Finasteride and dutasteride work by inhibiting 5-alpha-reductase, reducing DHT production by 60-70% and 90% respectively. Clinical trials published in the Journal of the American Academy of Dermatology show that finasteride stops progression in 83% of men and produces regrowth in 66% after two years.
But results take time. Six months minimum to see stabilization. Twelve months for visible regrowth. Why so slow? Because you’re not reversing damage instantly. You’re allowing miniaturized follicles to gradually recover over successive growth cycles.
Each growth cycle lasts months. A follicle needs multiple cycles under reduced DHT exposure to rebuild its dermal papilla, restore blood supply, and produce thicker hair. This is why dermatologists emphasize patience with DHT blockers.
Topical treatments like minoxidil work through a different mechanism (they don’t block DHT), but they’re often combined with finasteride for synergistic effects. Minoxidil extends anagen phase and improves blood flow, while finasteride removes the hormonal brake on follicle function.
Natural DHT blockers like saw palmetto and pumpkin seed oil show modest effects in studies, but they’re significantly weaker than pharmaceutical options. They may help maintain hair in early-stage loss but rarely produce dramatic regrowth.
The External Factors That Accelerate DHT Damage
DHT is the internal driver, but external factors determine how quickly the damage becomes visible. Think of it as a one-two punch: DHT weakens the follicle from the inside, while environmental stressors attack from the outside.
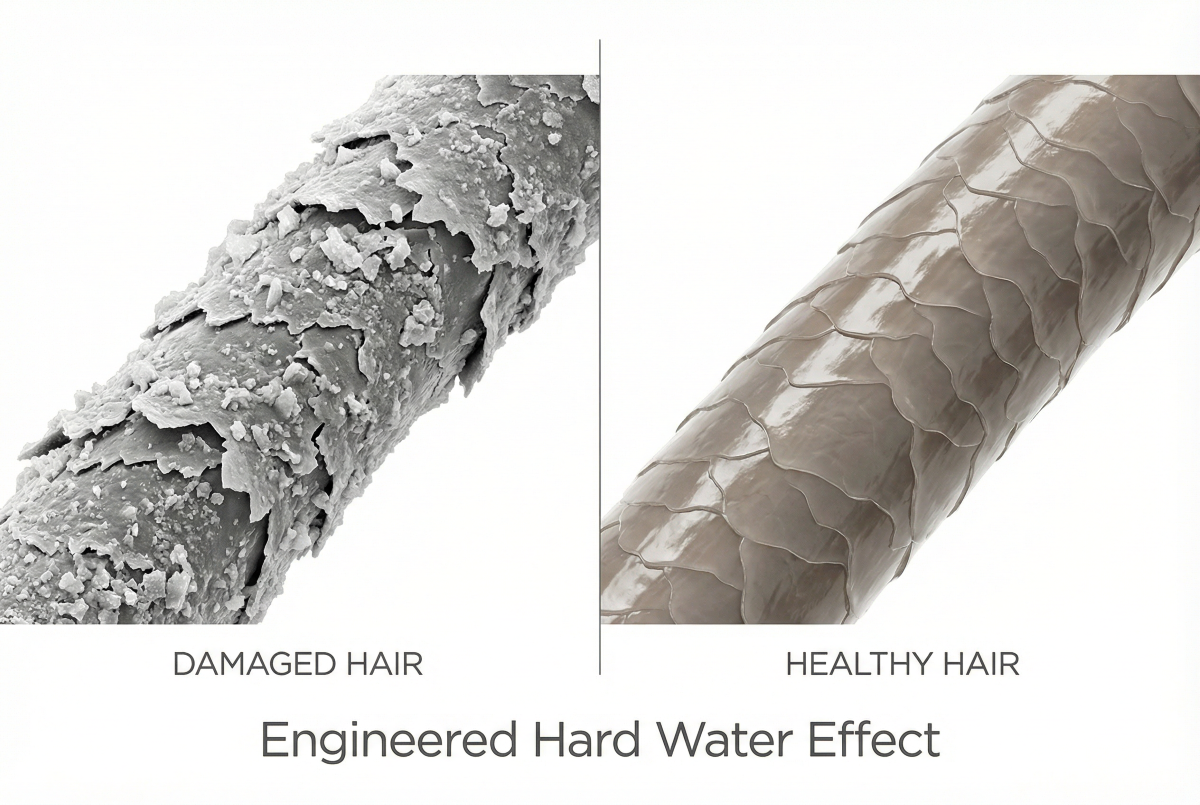
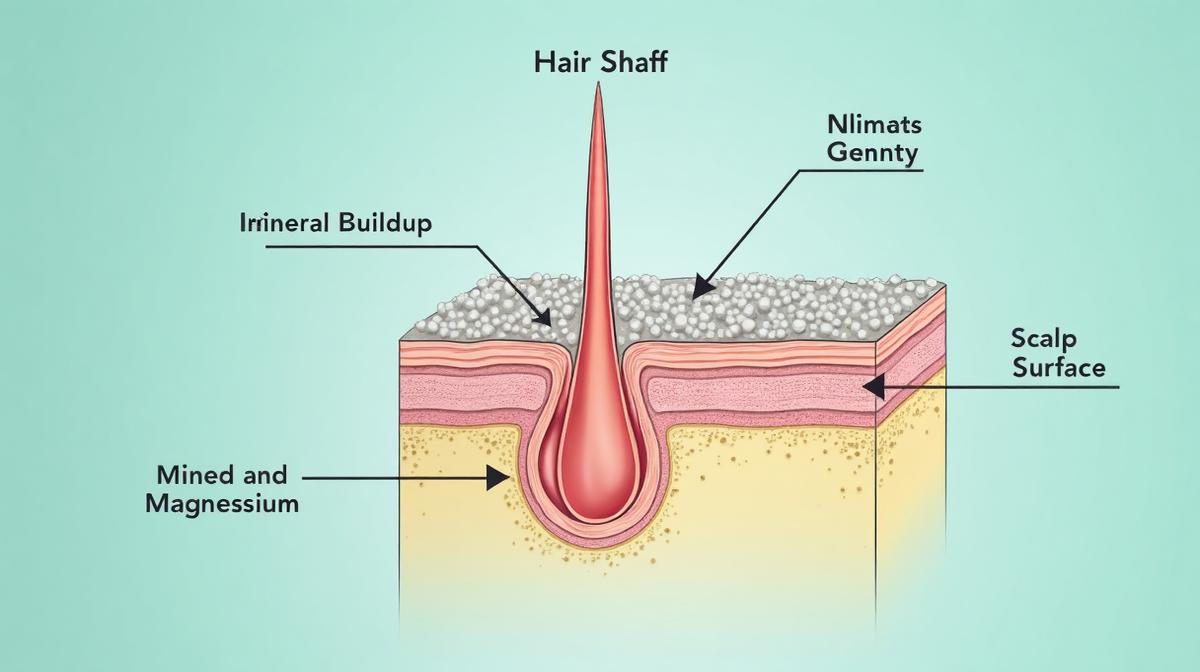
In the Gulf region, hard water is the primary external aggressor. High mineral content (calcium, magnesium, silica) creates a coating on the scalp and hair shaft that blocks nutrient absorption, clogs follicles, and creates chronic low-grade inflammation.
Miniaturized follicles are already fragile. When you add mineral buildup, you’re suffocating follicles that are barely hanging on. Research on hard water effects shows that mineral deposits change the scalp’s pH balance, increase oxidative stress, and impair the follicle’s ability to anchor hair shafts.
Harsh sulfate shampoos compound the problem by stripping the scalp’s protective lipid barrier, increasing sensitivity and inflammation. Your follicles are fighting DHT internally while dealing with chemical and mineral assault externally.
This is why a chelating shampoo like Regrowth+ is part of a complete hair loss strategy. It removes the mineral buildup that accelerates visible thinning, giving DHT-blocking treatments a cleaner environment to work in. You’re managing the external axis while pharmaceutical treatments manage the internal hormonal pathway.
Building a Complete DHT Management Strategy
Addressing DHT-driven hair loss requires a multi-axis approach. Pharmaceutical DHT blockers handle the hormonal mechanism. Topical treatments support follicle function. Environmental management removes external stressors.
Start with a dermatologist consultation to confirm androgenetic alopecia and rule out other causes (thyroid dysfunction, nutritional deficiencies, autoimmune conditions). Proper diagnosis is essential because treatments for DHT-driven loss won’t help if the underlying cause is different.
If androgenetic alopecia is confirmed, discuss finasteride or dutasteride. These are prescription medications with proven efficacy but potential side effects (sexual dysfunction in 1-2% of users, though most side effects resolve after discontinuation). Women of childbearing age cannot use these drugs due to birth defect risks.
Add environmental management: switch to a chelating shampoo to remove mineral buildup, avoid harsh sulfates, and protect your scalp from chlorine exposure. These changes won’t stop DHT, but they reduce the external factors that make thinning more visible and rapid.
Track progress with photos every three months. Hair loss treatment is measured in quarters and years, not weeks. Most people give up too early because they expect immediate results from a process that’s inherently gradual.
References
- 5-alpha-reductase isozymes and male pattern hair loss - Journal of Clinical Endocrinology & Metabolism
- Hair cycle dynamics in androgenetic alopecia - Dermatologic Therapy
- Androgen receptor distribution in human scalp - Journal of Investigative Dermatology
- Long-term efficacy of finasteride in male pattern hair loss - Journal of the American Academy of Dermatology