Your dermatologist just recommended a scalp biopsy. The word ‘biopsy’ triggers immediate anxiety, it sounds invasive, painful, maybe even dangerous. But here’s what’s actually happening: your doctor can’t determine the type of hair loss you have from visual examination alone. They need a tissue sample to see what’s destroying your follicles at the cellular level.
A scalp biopsy is the gold-standard diagnostic for distinguishing between scarring and non-scarring alopecia. It’s the difference between a condition that responds to treatment and one that causes permanent follicle destruction. The procedure takes about 15 minutes. Recovery is straightforward. And the information it provides can fundamentally change your treatment approach.
This isn’t a test your dermatologist orders casually. If they’re recommending it, they’ve already ruled out the obvious causes, environmental factors like hard water, nutritional deficiencies, hormonal imbalances. What remains requires microscopic analysis. Let’s walk through when it’s necessary, what actually happens during the procedure, and what the results can (and can’t) tell you.
This article contains affiliate links. See our affiliate disclosure for details.
When Your Dermatologist Orders a Scalp Biopsy
Not every case of hair loss requires a biopsy. Most don’t. If you’re experiencing diffuse thinning that started after moving to the Gulf region, your dermatologist will first check for hard water damage, thyroid dysfunction, or iron deficiency. These have clear diagnostic pathways that don’t require tissue sampling.
A biopsy becomes necessary when clinical examination and initial bloodwork don’t explain the pattern of loss. Specifically, dermatologists order scalp biopsies in these scenarios:
Suspected scarring alopecia. When you have patches of hair loss with visible scalp changes, redness, scaling, follicular plugging, or a smooth, shiny surface where follicles used to be, your doctor needs to confirm whether the follicles are permanently destroyed. Conditions like lichen planopilaris, frontal fibrosing alopecia, and central centrifugal cicatricial alopecia all cause scarring, but they require different treatment approaches. The biopsy reveals which inflammatory process is attacking the follicles.
Atypical presentation of common conditions. Sometimes alopecia areata doesn’t present as the classic round patches. Sometimes androgenetic alopecia affects unusual areas or progresses faster than expected. When the clinical picture doesn’t match the presumed diagnosis, a biopsy confirms what’s actually happening at the follicular level.
Treatment-resistant hair loss. You’ve tried minoxidil for six months. You’ve corrected nutritional deficiencies. You’ve switched to dermatologist-recommended hair care. Nothing’s working. A biopsy can reveal underlying inflammatory processes or miniaturization patterns that explain why standard treatments aren’t effective.
The key distinction: a scalp biopsy diagnoses the type of hair loss, not the cause. It won’t tell you that stress triggered your alopecia areata or that hormones are driving your androgenetic alopecia. It shows what’s happening to your follicles right now, inflammation, miniaturization, scarring, or autoimmune attack. The ‘why’ still requires clinical correlation with your medical history, bloodwork, and environmental factors.
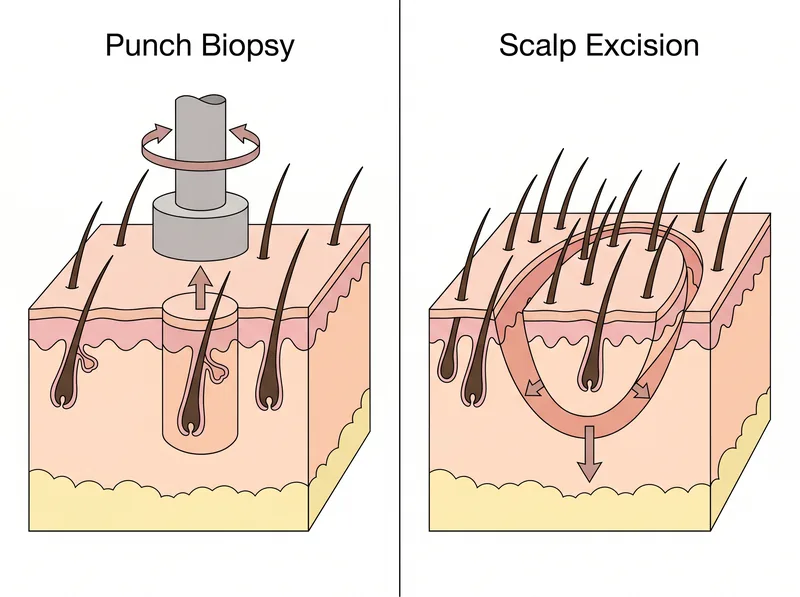 Two main scalp biopsy techniques: punch biopsy (left) extracts a cylindrical tissue sample, while scalp excision (right) removes an elliptical section for deeper analysis.
Two main scalp biopsy techniques: punch biopsy (left) extracts a cylindrical tissue sample, while scalp excision (right) removes an elliptical section for deeper analysis.
The Two Types of Scalp Biopsy Procedures
Dermatologists use two main techniques, chosen based on what they’re trying to diagnose:
Punch biopsy. This is the most common approach. Your dermatologist uses a circular punch tool (typically 4mm in diameter, about the size of a pencil eraser) to extract a cylindrical core of tissue that includes the epidermis, dermis, and subcutaneous fat where the follicle bulbs reside. The tool rotates as it cuts, creating a clean circular wound. The tissue sample is then lifted out with forceps.
Punch biopsies are fast, the actual tissue extraction takes less than 30 seconds. They’re performed under local anesthetic (you’ll feel pressure but no pain during the procedure). Most dermatologists take two punch biopsies from different areas of the scalp: one from an active area of hair loss and one from the edge of a patch where follicles are still present. This comparison helps identify the stage and progression of the condition.
Scalp excision biopsy. Less common but sometimes necessary for diagnosing scarring alopecias. The dermatologist removes an elliptical (football-shaped) section of scalp tissue, which provides a larger sample and preserves the natural orientation of hair follicles. This technique is preferred when the suspected condition requires analysis of follicle distribution patterns or when the dermatopathologist needs to see multiple follicles in their natural arrangement.
Excision biopsies require sutures (usually 3-5 stitches) and leave a linear scar, but the scar is typically hidden within existing hair. The procedure takes slightly longer, about 20-30 minutes including suturing, but provides more diagnostic information for complex cases.
Your dermatologist will explain which technique they’re using and why. If you have long hair, they’ll select a site that can be easily covered during healing. If you have very short hair or are bald in the biopsy area, they’ll discuss scar visibility and placement options.
What Happens During the Procedure
Let’s walk through a standard punch biopsy, which is what most patients experience:
You’ll sit in the exam chair while your dermatologist identifies the biopsy site. They’ll mark it with a surgical pen. If you have hair in that area, they’ll trim a small section (about the size of a quarter) to expose the scalp. This isn’t a full shave, just enough to access clean skin.
Local anesthetic comes next. The injection stings for about 5-10 seconds, similar to a dental numbing shot. Some dermatologists use a topical numbing cream first to reduce injection discomfort, but this adds 20-30 minutes to the appointment for the cream to take effect. The local anesthetic works within 1-2 minutes. You’ll feel pressure and tugging during the biopsy, but no sharp pain.
The actual biopsy: your dermatologist positions the punch tool perpendicular to your scalp and rotates it while applying gentle downward pressure. You’ll hear a slight crunching sound as it cuts through tissue, that’s normal. Once the tool reaches the subcutaneous layer, they remove it and use forceps to lift the cylindrical tissue sample. If they’re taking two samples, they repeat the process at the second site.
Hemostasis (stopping the bleeding) takes a few minutes. Your dermatologist will apply pressure with gauze, possibly use an aluminum chloride solution to constrict blood vessels, or place a single suture if the wound is larger than 4mm. Most punch biopsies don’t require stitches, the circular wound is small enough to heal on its own. You’ll leave with a small bandage and aftercare instructions.
Total time in the office: 20-30 minutes for a punch biopsy, 40-50 minutes for an excision biopsy. The tissue samples are placed in formalin (a preservative) and sent to a dermatopathology lab for analysis. Results typically return in 7-14 days.
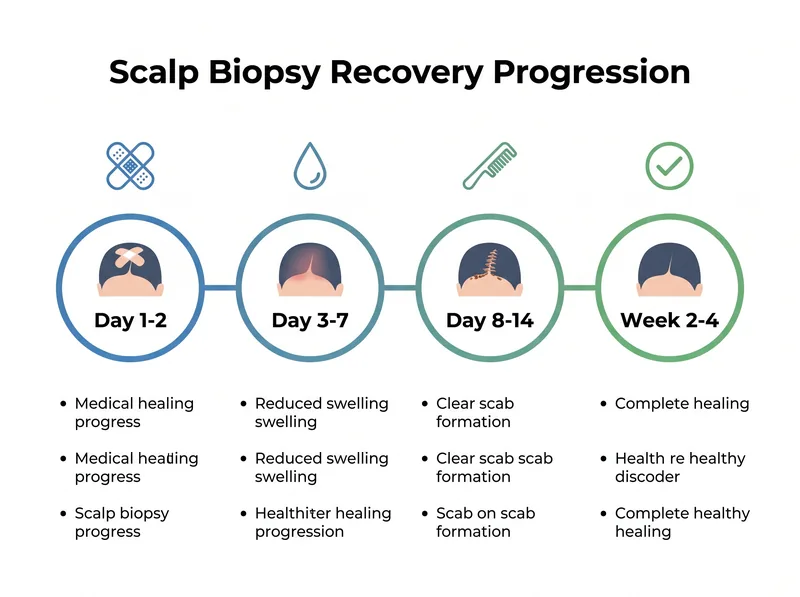 Typical recovery timeline following scalp biopsy: most patients experience complete surface healing within 10-14 days, with final results available in 2-3 weeks.
Typical recovery timeline following scalp biopsy: most patients experience complete surface healing within 10-14 days, with final results available in 2-3 weeks.
Recovery and Aftercare Expectations
The first 24-48 hours require the most attention. Keep the bandage dry and in place. No hair washing for 48 hours minimum, your dermatologist will specify the exact timeline based on the biopsy type and whether you have sutures. If you’re in the Gulf region with hard water, this is actually an opportunity to minimize exposure; when you do resume washing, consider using a chelating shampoo like Regrowth+ to prevent mineral buildup around the healing site.
Days 3-7: The biopsy site will form a scab. This is normal healing. Do not pick at it. You can gently wash your hair around the area (not directly on it) starting on day 3-4, depending on your doctor’s instructions. Use lukewarm water and avoid aggressive scrubbing. Pat dry, don’t rub.
Some patients experience mild throbbing or tenderness for 2-3 days. Over-the-counter pain relievers (acetaminophen or ibuprofen) are usually sufficient. If you’re experiencing severe pain, increasing redness, warmth, or discharge from the site, contact your dermatologist immediately, these are signs of infection, though infection rates are very low (less than 1% in published case series).
Days 8-14: The scab will naturally fall off. Don’t force it. Underneath, you’ll see pink healing skin. If you had sutures, your dermatologist will remove them around day 7-10. The removal process is quick and causes minimal discomfort, usually just a slight pulling sensation.
Week 2-4: The biopsy site continues to heal. The pink color gradually fades to match your surrounding scalp. For punch biopsies, the small circular scar becomes nearly invisible, especially if you have hair covering it. For excision biopsies, the linear scar may remain slightly visible but typically blends into the natural scalp contours.
Hair regrowth at the biopsy site: This varies. Some patients see hair regrowth within 2-3 months. Others develop a small permanent bald spot at the exact biopsy location, particularly if the biopsy was taken from an area already affected by scarring alopecia. Your dermatologist will discuss this possibility before the procedure.
What the Biopsy Results Actually Reveal
The dermatopathologist examines your tissue sample under a microscope and looks for specific patterns. Here’s what they can identify:
Follicle miniaturization patterns. In androgenetic alopecia, follicles progressively shrink. The pathologist measures the ratio of terminal (thick) hairs to vellus (fine) hairs. A ratio below 3:1 indicates significant miniaturization. They also assess whether the miniaturization is uniform (typical of androgenetic alopecia) or patchy (suggesting another process).
Inflammatory infiltrates. The presence, type, and location of inflammatory cells distinguish between different scarring alopecias. Lichen planopilaris shows lymphocytic inflammation around the upper follicle. Discoid lupus shows interface dermatitis. Central centrifugal cicatricial alopecia shows premature desquamation of the inner root sheath. These are distinct cellular signatures that clinical examination can’t differentiate.
Fibrosis and scarring. The pathologist determines whether follicles are being replaced by fibrous tissue (scarring). This is the critical distinction between reversible and permanent hair loss. Scarred follicles cannot regrow hair. Non-scarred follicles, even if dormant or miniaturized, retain the potential for regrowth with appropriate treatment.
Autoimmune markers. In alopecia areata, the pathologist identifies a characteristic ‘swarm of bees’ pattern, lymphocytes clustering around the follicle bulb. This confirms autoimmune attack rather than other causes of patchy hair loss.
What the biopsy cannot reveal: It won’t identify nutritional deficiencies (bloodwork does that). It won’t diagnose hormonal imbalances (again, bloodwork). It won’t tell you whether stress or environmental factors triggered your hair loss (that requires clinical history). The biopsy shows the current state of your follicles and the pathological process affecting them. The ‘why’ still requires your dermatologist to integrate the biopsy findings with your complete medical picture.
Results are typically reported in a formal pathology report that your dermatologist will review with you. The report includes microscopic findings, a diagnosis, and sometimes recommendations for additional testing or treatment approaches. This is when you’ll discuss next steps based on what the biopsy revealed.
Risks, Limitations, and When to Seek Alternatives
Scalp biopsy is generally safe, but no procedure is risk-free. Understand what can go wrong:
Infection. Rare (less than 1% of cases) but possible. Signs include increasing pain, redness spreading beyond the biopsy site, warmth, swelling, or pus. If you notice these symptoms, contact your dermatologist immediately. Most infections respond quickly to oral antibiotics.
Bleeding. Some oozing in the first 24 hours is normal. Persistent bleeding beyond 48 hours or bleeding that soaks through bandages requires medical attention. Patients on blood thinners (aspirin, warfarin, other anticoagulants) have higher bleeding risk, discuss this with your dermatologist before the procedure. You may need to temporarily stop certain medications.
Scarring. All biopsies create scars. Punch biopsies leave small circular scars (usually 4mm or less) that are often invisible once healed, especially if covered by hair. Excision biopsies leave linear scars. In patients with darker skin types or keloid tendency, there’s a risk of hypertrophic scarring or keloid formation. Your dermatologist should assess this risk before proceeding.
Diagnostic limitations. Sometimes the biopsy doesn’t provide a definitive answer. The tissue sample might not capture the active area of disease, or the findings might be non-specific. In these cases, your dermatologist may recommend a second biopsy from a different site or additional diagnostic tests like trichoscopy.
When to consider alternatives: If you have a bleeding disorder, active scalp infection, or extreme needle phobia, discuss options with your dermatologist. In some cases, non-invasive diagnostics like trichoscopy or phototrichogram can provide sufficient information without tissue sampling. However, these techniques can’t definitively diagnose scarring alopecia, they can only suggest it.
The decision to proceed with a scalp biopsy should be made collaboratively. Ask your dermatologist: What specific question are we trying to answer? Will the biopsy results change my treatment plan? What happens if we don’t do the biopsy? A good dermatologist will explain their clinical reasoning and help you weigh the diagnostic value against the minor risks and discomfort of the procedure.
References
- Scalp Biopsy: Diagnosis and Treatment of Hair Disorders - PubMed - Journal of the American Academy of Dermatology
- Horizontal vs Vertical Scalp Biopsy Sections: Diagnostic Accuracy - PubMed - International Journal of Trichology
- Hair Loss: Diagnosis and Treatment - American Academy of Dermatology
- Scarring Alopecia: Pathogenesis and Clinical Features - PubMed Central