Your hairdresser says your hair is getting thinner. Your dermatologist says you’re losing density. Are they talking about the same thing?
No. And the confusion between these two terms causes people to misdiagnose their own hair loss and choose the wrong treatments.
Hair density measures how many follicles you have per square centimeter of scalp. Hair thickness measures the diameter of each individual strand. You can have high density with fine strands. You can have low density with thick strands. They’re independent variables that change at different rates as you age.
Here’s what actually matters: density determines how much scalp shows through. Thickness determines how much volume each strand contributes. Both affect how your hair looks, but they respond to completely different interventions. Understanding which one you’re losing, or if you’re losing both, changes everything about how you should respond.
This article contains affiliate links. See our affiliate disclosure for details.
What Hair Density Actually Measures
Density is a population count. It’s the number of active hair follicles in a defined area of your scalp, typically measured per square centimeter.
Average density varies by ethnicity and natural hair color. People of Asian descent average 150-175 follicles/cm². People of European descent average 120-150 follicles/cm². People of African descent average 100-120 follicles/cm². Redheads typically have lower density (around 90 follicles/cm²) but compensate with thicker individual strands.
You’re born with all the follicles you’ll ever have. You can’t create new ones. Density loss happens when follicles miniaturize (shrink and stop producing visible hair) or when follicles enter extended resting phases and don’t cycle back to growth.
This is why understanding the hair growth cycle matters so much. A follicle that’s temporarily dormant isn’t lost, it can potentially be reactivated. A miniaturized follicle that’s been dormant for years? Much harder to rescue.
Density loss shows up as widening parts, more visible scalp, and a general “see-through” quality to your hair, especially under harsh lighting or when wet. You’re not losing volume per strand, you’re losing the number of strands covering each section of scalp.
 Density counts follicles in a defined scalp area, while thickness measures the width of individual strands, two completely independent variables.
Density counts follicles in a defined scalp area, while thickness measures the width of individual strands, two completely independent variables.
What Hair Thickness Actually Measures
Thickness is the diameter of each individual hair shaft, measured in microns (μm). It has nothing to do with how many hairs you have.
Fine hair: 40-60 μm. Medium hair: 60-80 μm. Coarse hair: 80-120 μm. The thickest human hair strands can reach 180 μm.
Strand thickness is determined by the size of your hair follicle and the rate of keratin deposition during the growth phase. Genetics set your baseline, but thickness can decline due to hormonal changes, nutritional deficiencies, or damage to the follicle’s keratin production mechanism.
When strand thickness declines, you lose volume and body. Your hair feels limp. Ponytails get thinner. But your part might look exactly the same because you haven’t lost follicles, each follicle is just producing a narrower strand.
This is the distinction most people miss. Thinning hair (reduced strand diameter) feels different from hair loss (reduced follicle count). The first affects texture and volume. The second affects coverage.
Why They Decline Independently
Density and thickness are controlled by different biological mechanisms. That’s why they don’t always move together.
Density is primarily affected by hormones (especially DHT in androgenetic alopecia), autoimmune conditions, inflammatory scalp disorders, and aging-related follicle miniaturization. When DHT binds to follicle receptors, it progressively shrinks the follicle until it stops producing visible hair. That’s density loss.
Thickness is affected by keratin synthesis, nutritional status (especially protein, iron, and B vitamins), thyroid function, and physical damage to the hair shaft. A healthy follicle can produce a thinner strand if it’s not getting adequate building blocks or if hormonal signals are changeing keratin production.
You can lose density while maintaining thickness. This happens in early androgenetic alopecia when follicles miniaturize but the remaining follicles are still producing normal-diameter strands. Your part widens, but the hair you have left feels thick.
You can lose thickness while maintaining density. This happens with nutritional deficiencies, hypothyroidism, or after periods of extreme stress. You still have all your follicles, but each one is producing a finer strand. Your coverage looks okay, but your ponytail is half its normal diameter.
And yes, you can lose both simultaneously. That’s the worst-case scenario, fewer follicles, each producing thinner strands. This is common in advanced androgenetic alopecia, chronic telogen effluvium, or severe nutritional deficiency.
 Density and thickness follow different decline curves, you can lose follicles while maintaining thick strands, or vice versa.
Density and thickness follow different decline curves, you can lose follicles while maintaining thick strands, or vice versa.
How to Measure Each One at Home
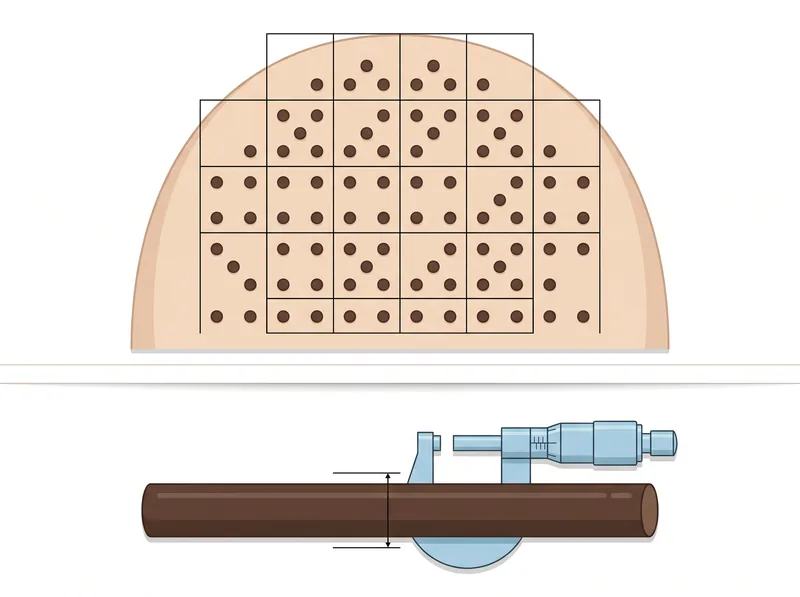
Measuring density requires counting follicles in a defined area. Part your hair in sections and use your phone camera with macro mode to photograph your scalp. Draw a 1cm x 1cm grid on the photo using any photo editing app. Count the visible follicle openings (the tiny dots where hair emerges). Multiply by 100 to get follicles per 10cm².
This method isn’t perfectly accurate, professional trichoscopy uses magnification and specialized lighting, but it’s good enough to track changes over time. Take photos in the same lighting, same part location, every 3-6 months.
Measuring thickness is harder without tools. The ponytail test gives you a rough proxy: measure the circumference of your ponytail at the same point (mid-length, not at the elastic). A declining circumference over time usually indicates thickness loss, assuming density is stable.
For actual diameter measurement, you need a micrometer. Pluck a few strands from different areas of your scalp (not cut ends, plucked roots). Measure the diameter at the midpoint of each strand. Average the measurements. Anything under 60 μm is fine hair. Over 80 μm is coarse.
Track both metrics separately. If density is dropping but thickness is stable, you’re dealing with follicle miniaturization (likely hormonal). If thickness is dropping but density is stable, you’re dealing with keratin production issues (likely nutritional or systemic). If both are dropping, you need a complete intervention.
What Causes Density Loss
Androgenetic alopecia (pattern hair loss) is the #1 cause of density loss. DHT-sensitive follicles progressively shrink. The growth phase shortens. Eventually the follicle produces only vellus hair (the fine, nearly invisible fuzz). From a distance, it looks like the follicle disappeared.
Chronic inflammation is the second major cause. Scalp conditions like seborrheic dermatitis, psoriasis, or folliculitis create an inflammatory environment that changes follicle cycling. Follicles get stuck in resting phase or miniaturize prematurely.
Autoimmune conditions (alopecia areata, frontal fibrosing alopecia, lichen planopilaris) directly attack follicles. The immune system targets follicle structures, causing sudden density loss in patches or along the hairline.
Aging alone causes density loss even without androgenetic alopecia. Follicle stem cells have a limited number of division cycles. As you age, more follicles exhaust their regenerative capacity and stop cycling. This is why even people without genetic hair loss see some thinning after 50.
In the Gulf region, hard water exposure can accelerate density loss by creating chronic scalp inflammation and mineral buildup that changes follicle function. Using a chelating shampoo like Regrowth+ to remove mineral deposits can help maintain a healthier scalp environment and potentially slow follicle miniaturization.
What Causes Thickness Loss
Nutritional deficiency is the most reversible cause. Inadequate protein intake limits keratin synthesis. Iron deficiency (even without anemia) reduces oxygen delivery to follicles, slowing keratin production. B vitamin deficiencies change cellular metabolism in the follicle.
Thyroid dysfunction, both hypo and hyperthyroidism, affects strand thickness. Thyroid hormones regulate keratin gene expression. When thyroid function is off, follicles produce thinner, more brittle strands even though follicle count remains normal.
Hormonal fluctuations during pregnancy, postpartum, and menopause can temporarily reduce strand diameter. Estrogen promotes keratin synthesis. When estrogen drops, so does strand thickness. This is why postpartum hair changes often include both shedding (density) and texture changes (thickness).
Physical damage to the hair shaft, heat styling, chemical treatments, mechanical stress, doesn’t change the diameter at the root, but it can cause breakage and splitting that makes strands appear thinner. This is structural damage, not biological thickness loss.
Chronic stress improves cortisol, which can change keratin synthesis. Follicles shift resources toward survival functions and away from cosmetic functions like producing thick hair. The effect is subtle but measurable over months of sustained stress.
Why the Distinction Changes Treatment Strategy
If you’re losing density, you need interventions that prevent follicle miniaturization or reactivate dormant follicles. That means minoxidil (extends growth phase, stimulates follicle activity), DHT blockers (finasteride, dutasteride, or natural alternatives), anti-inflammatory scalp treatments, and possibly microneedling to stimulate follicle stem cells.
If you’re losing thickness, you need interventions that support keratin synthesis. That means improving protein intake, correcting nutritional deficiencies (iron, B12, biotin, zinc), managing thyroid function, and reducing physical/chemical damage to the hair shaft.
Using a hair growth shampoo when you’re only losing thickness? Probably won’t help. The follicles are fine, they just need better nutritional support. Conversely, taking biotin supplements when you’re losing density due to androgenetic alopecia? Also won’t help. Biotin supports keratin production, not follicle survival.
This is why complete bloodwork matters. You need to know if you’re dealing with a hormonal issue (density), a nutritional issue (thickness), or both. Treating the wrong variable wastes time and money.
Most people over 40 are dealing with both to some degree. That’s when you need a multi-pronged approach: address follicle miniaturization AND support keratin production. But you still need to know which one is the primary driver so you can prioritize interventions.
What Normal Age-Related Changes Look Like
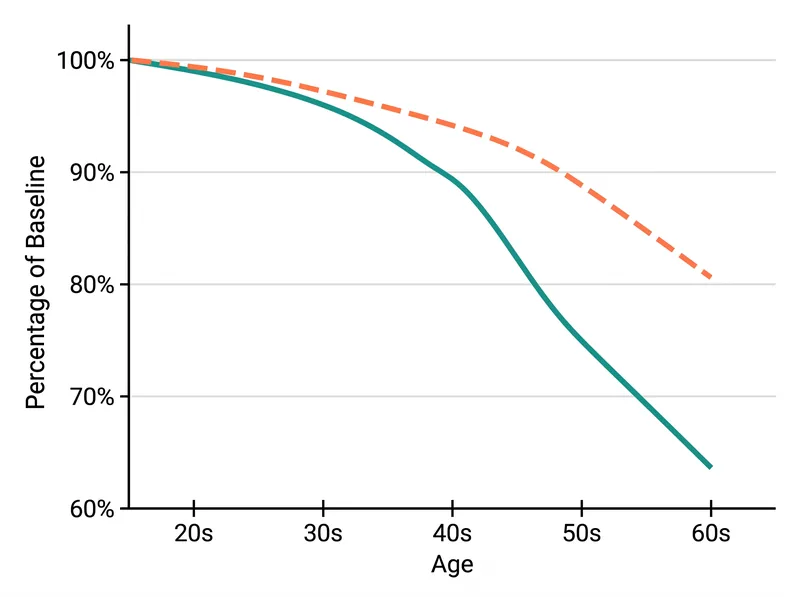
Between ages 20-30: density remains stable or increases slightly as late-developing follicles mature. Strand thickness is at lifetime peak.
Between ages 30-40: density begins gradual decline (approximately 5-10% loss per decade). Strand thickness remains relatively stable in most people.
Between ages 40-50: density loss accelerates (10-15% per decade). Strand thickness begins noticeable decline, especially in women approaching menopause.
Between ages 50-60: density loss continues (another 10-15%). Strand thickness declines more noticeably due to hormonal changes and cumulative nutritional/environmental factors.
After age 60: both density and thickness are significantly reduced compared to peak. The rate of loss slows somewhat, but the cumulative effect is substantial. Most people have lost 30-40% of peak density and 20-30% of peak strand thickness by age 65.
These are averages. Genetics, ethnicity, hormonal factors, and environmental exposures create huge individual variation. But the pattern is consistent: density starts declining first, thickness follows 10-15 years later, and both accelerate after 40.
References
- Ethnic Variation in Hair Follicle Density - Journal of Investigative Dermatology
- Hair Shaft Diameter Variation and Clinical Implications - PubMed Central
- Age-Related Hair Loss and Changes - American Academy of Dermatology
- Thyroid Disorders and Hair Changes - Mayo Clinic
- Nutritional Factors in Hair Structure - Dermatology and Therapy Journal