This article contains affiliate links. See our affiliate disclosure for details.
You found a clump of your teenager’s hair in the shower drain. Again. Their ponytail looks thinner than it did six months ago. And now they’re asking if something’s wrong with their hair.
Here’s the thing: teenage hair loss is more common than most parents realize. But it’s also more complicated. Some shedding during adolescence is completely normal, driven by the same hormonal surges that cause acne and growth spurts. Other patterns signal nutritional deficiencies, autoimmune conditions, or psychological stress that needs immediate attention.
The difference isn’t always obvious. A 15-year-old girl losing 150 hairs per day might be experiencing normal telogen effluvium triggered by exam stress. Or she might have iron-deficiency anemia that’s been silently progressing for months. A 16-year-old boy noticing temple recession could be seeing early male pattern baldness, or he could have traction alopecia from tight athletic headgear.
This guide walks through the physiological reasons teenagers shed hair, the warning signs that distinguish normal from concerning, and when pediatric dermatology becomes the right specialty. We’ll cover hormonal patterns, nutritional red flags, stress-induced shedding, and the eating disorder connection that most parents miss. Because when it comes to adolescent hair loss, the difference between watching and acting can determine whether the problem resolves on its own or requires intervention.
Why Teenagers Lose Hair: The Puberty Connection
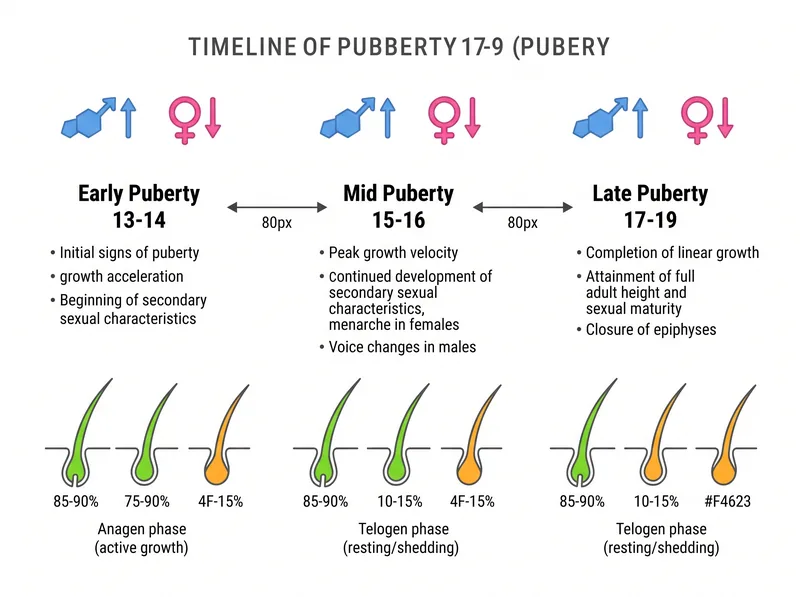
Puberty rewires the entire endocrine system. Between ages 12 and 18, teenagers experience hormonal fluctuations more dramatic than anything they’ll face until pregnancy or menopause. These surges directly affect hair follicles.
Androgens (testosterone and DHT) increase in both boys and girls during puberty. In genetically susceptible individuals, DHT binds to follicle receptors and miniaturizes hair shafts. This is the same mechanism behind adult male pattern baldness, but in teenagers it usually manifests as subtle temple recession or crown thinning rather than full baldness.
Estrogen levels also fluctuate wildly, particularly in girls. Estrogen prolongs the anagen (growth) phase of hair, so when levels drop (during menstrual cycles or in conditions like PCOS), more follicles shift into telogen (shedding) phase simultaneously. This creates the appearance of sudden hair loss, even though it’s just synchronized shedding.
According to research published in the Journal of Clinical Endocrinology & Metabolism, approximately 12% of adolescent girls experience temporary telogen effluvium during peak puberty years. Most cases resolve within 6-9 months as hormone levels stabilize.
But here’s what confuses parents: normal pubertal shedding looks identical to pathological hair loss. Both cause increased hair in the brush, visible scalp, and thinner ponytails. The difference is timing, pattern, and associated symptoms.
 Hormonal fluctuations during puberty can temporarily change normal hair growth cycles, leading to increased shedding that often resolves naturally.
Hormonal fluctuations during puberty can temporarily change normal hair growth cycles, leading to increased shedding that often resolves naturally.
Normal Teenage Shedding vs. Concerning Patterns
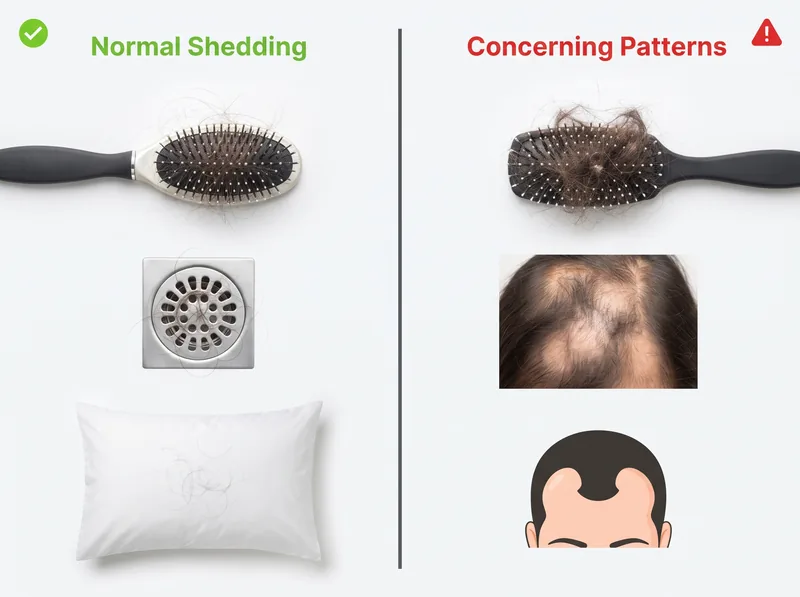
Normal adolescent shedding has specific characteristics. It’s diffuse (all over the scalp, not in patches), temporary (peaks and resolves within 3-6 months), and proportional to a triggering event like starting menstruation, rapid growth, or exam stress.
You’ll see 50-150 hairs per day in the shower, on the pillow, and in the brush. The hairline remains intact. There’s no scalp inflammation, no itching, no pain. And critically, the teenager’s overall health is fine. They’re eating normally, maintaining weight, and functioning at school.
Concerning patterns look different. Circular bald patches (alopecia areata) signal an autoimmune process. Broken hairs at the scalp line with ‘exclamation point’ appearance also indicate alopecia areata. A receding frontal hairline in girls under 16 is unusual and warrants evaluation.
Diffuse thinning accompanied by fatigue, cold intolerance, or weight changes suggests thyroid dysfunction. Hair loss plus irregular or absent periods points to PCOS or hypothalamic amenorrhea. Scalp tenderness, scaling, or pustules indicate infection or inflammatory conditions like scalp psoriasis.
The American Academy of Dermatology identifies these red flags: hair loss lasting longer than 6 months, bald patches larger than a quarter, scalp symptoms (pain, redness, scaling), or hair loss accompanied by systemic symptoms (fatigue, weight loss, menstrual irregularities). Any of these warrant a dermatology consultation.
Timing matters too. Hair loss that starts abruptly and worsens rapidly over 2-3 months is more concerning than gradual thinning over a year. Sudden onset suggests a specific trigger (medication, infection, nutritional crash) that needs identification.
The Eating Disorder and Restrictive Diet Connection
This is the pattern pediatric dermatologists see most often, and the one parents miss most frequently. Hair loss in teenagers with eating disorders presents 3-6 months after caloric restriction begins. By the time parents notice thinning hair, the nutritional deficiency is advanced.
Hair follicles are metabolically expensive. They require constant protein synthesis, iron transport, and energy availability. When caloric intake drops below maintenance levels, the body triages resources toward vital organs. Hair growth shuts down first.
Anorexia nervosa, bulimia, orthorexia, and restrictive ‘clean eating’ all cause telogen effluvium. So do high-restriction diets popular among teenagers: keto without adequate protein, veganism without B12 supplementation, juice cleanses, intermittent fasting taken to extremes.
The hair loss pattern is diffuse and dramatic. Teenagers can lose 30-50% of hair density in 4-6 months. But here’s the insidious part: the hair loss starts months after the restriction begins, so the connection isn’t obvious. Parents attribute it to stress or hormones, not realizing their teenager has been eating 800 calories per day.
According to a study in the International Journal of Eating Disorders, 57% of adolescents with anorexia nervosa experience significant hair loss. Recovery requires both nutritional rehabilitation and psychological treatment. Hair regrowth typically begins 3-4 months after normal eating resumes.
Warning signs beyond hair loss: preoccupation with food, calorie counting, excessive exercise, avoidance of family meals, wearing baggy clothes, cold intolerance, fine body hair (lanugo), dizziness, and menstrual irregularities. If hair loss coincides with any of these, eating disorder evaluation is urgent.
 Recognizing the difference between normal shedding and patterns that warrant professional evaluation can help parents make informed decisions about seeking care.
Recognizing the difference between normal shedding and patterns that warrant professional evaluation can help parents make informed decisions about seeking care.
Nutritional Deficiencies That Cause Teen Hair Loss
Even without disordered eating, teenagers have higher nutritional needs than adults and lower dietary quality. Growth spurts, menstruation, athletic training, and erratic eating habits create perfect conditions for deficiency.
Iron deficiency is the most common culprit. Teenage girls lose iron through menstruation. Teenage athletes lose it through foot-strike hemolysis and increased red blood cell production. Vegetarians and vegans struggle to absorb non-heme iron. Research shows that ferritin levels below 40 ng/mL impair hair growth, even when hemoglobin is normal.
The problem: standard blood tests check hemoglobin, not ferritin. A teenager can have ‘normal’ iron levels (hemoglobin 12-14 g/dL) but depleted iron stores (ferritin under 20 ng/mL). Their doctor says iron is fine, but their hair keeps falling out. This is why ferritin testing matters for unexplained hair loss.
Zinc deficiency presents with hair loss, white spots on nails, and poor wound healing. It’s common in teenagers who eat primarily processed foods with low bioavailable zinc. Vitamin D deficiency (endemic in the Gulf region due to sun avoidance) changes the hair growth cycle. B12 deficiency affects vegetarians and those with absorption issues.
Protein deficiency causes hair to become thin, brittle, and depigmented before falling out. Teenagers need 0.85-1.0 grams of protein per kilogram body weight daily. A 55kg teenager needs 47-55 grams. One chicken breast, two eggs, and a cup of Greek yogurt barely meet that. Many teenagers subsist on cereal, pasta, and snacks with minimal protein.
The solution isn’t random supplementation. It’s targeted testing (ferritin, vitamin D, B12, zinc) followed by therapeutic supplementation at higher doses than typical multivitamins provide. Iron supplementation for hair loss typically requires 65mg elemental iron daily for 3-6 months. That’s 3-4 times the amount in a standard multivitamin.
Stress, Anxiety, and Trichotillomania in Adolescents
Psychological stress triggers hair loss through two distinct mechanisms. The first is telogen effluvium: chronic stress signals follicles to enter resting phase prematurely. The second is trichotillomania: compulsive hair pulling driven by anxiety or obsessive-compulsive tendencies.
Telogen effluvium from stress peaks 2-3 months after the stressor begins. Exam periods, social conflicts, family changeion, or chronic academic pressure all qualify. The teenager sheds 150-300 hairs per day for several months, then recovery begins as stress resolves. Total cycle: 6-9 months from trigger to regrowth.
Trichotillomania looks different. Hair loss is patchy and irregular, concentrated in easily reached areas: frontal scalp, crown, eyebrows. Broken hairs of varying lengths create a ‘moth-eaten’ appearance. The scalp itself is healthy with no inflammation. Many teenagers pull hair unconsciously during homework, screen time, or before sleep.
According to the American Academy of Dermatology, trichotillomania affects 1-2% of adolescents, with peak onset between ages 11-13. It’s classified as an impulse control disorder related to OCD. Treatment requires cognitive behavioral therapy, specifically habit reversal training.
Parents often mistake trichotillomania for alopecia areata because both create patchy loss. The distinction: trichotillomania shows hairs of different lengths (because they’re pulled at different times), while alopecia areata shows smooth bald patches with no hair at all. A dermatologist can differentiate them immediately.
Stress-related hair loss in teenagers warrants mental health evaluation, not just dermatological treatment. If hair pulling is compulsive, therapy is first-line treatment. If shedding is stress-induced, addressing the underlying anxiety or depression is essential. Hair regrowth follows psychological improvement.
When to See a Pediatric Dermatologist
Pediatric dermatology becomes appropriate when hair loss persists beyond 6 months, creates bald patches, or occurs alongside systemic symptoms. General pediatricians can order initial bloodwork, but dermatologists have diagnostic tools most primary care offices lack.
Trichoscopy (magnified scalp examination) differentiates between scarring and non-scarring alopecia, identifies miniaturized hairs characteristic of androgenetic alopecia, and detects broken hairs indicative of trichotillomania or fungal infection. A 5-minute trichoscopy provides more diagnostic information than months of observation.
Dermatologists also perform hair pull tests quantitatively. In a normal scalp, fewer than 3 hairs per 60-hair pull come out. In active telogen effluvium, 10-15 hairs release. This objective measurement distinguishes normal shedding from pathological loss.
Scalp biopsy is reserved for unclear cases or suspected scarring alopecia. Conditions like frontal fibrosing alopecia and lichen planopilaris can present in late adolescence. Early diagnosis prevents permanent follicle destruction.
The consultation should include complete medical history (medications, recent illness, diet changes, stress events), family history of hair loss, menstrual history for girls, and physical examination of scalp, hair, and nails. Initial bloodwork typically includes CBC, ferritin, vitamin D, TSH, and possibly testosterone/DHEA-S if PCOS is suspected.
Don’t wait for ‘significant’ hair loss. If you’re noticing it, it’s significant. Teenagers have already lost 30-40% of hair density by the time thinning becomes visibly obvious. Earlier intervention means better outcomes.
Environmental Factors in the Gulf Region
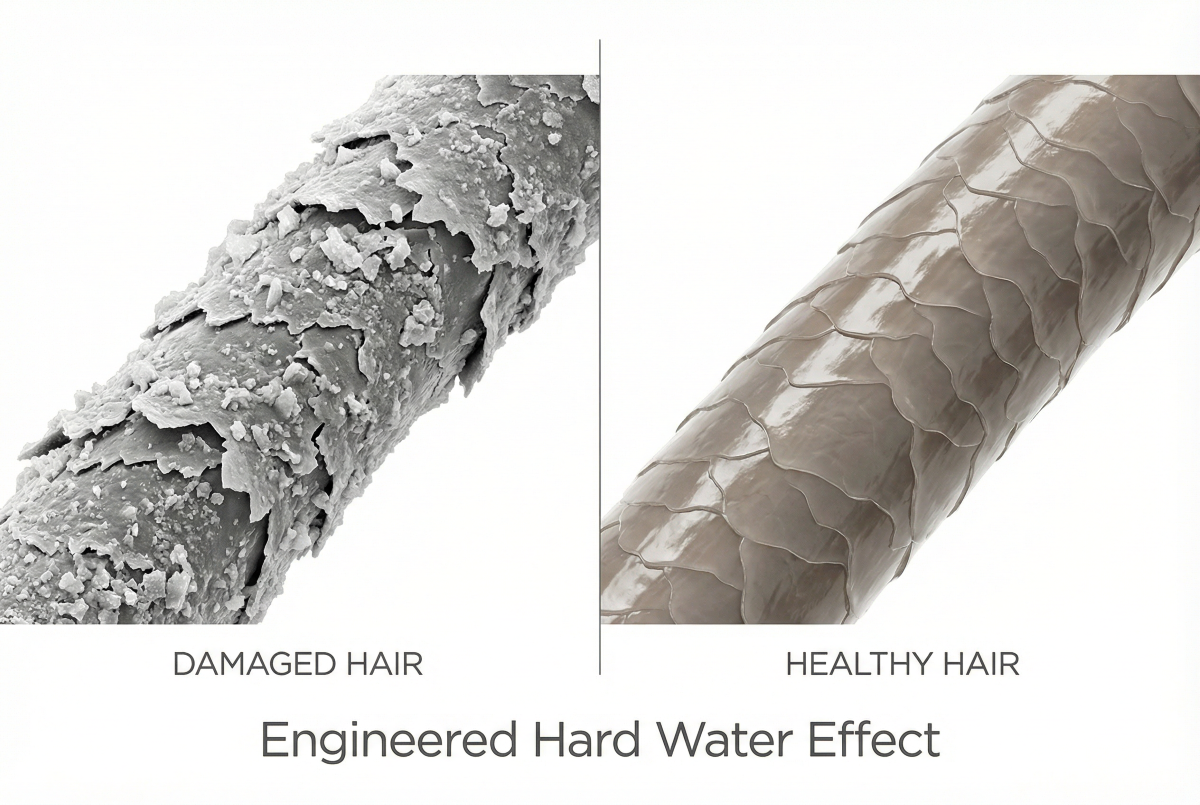
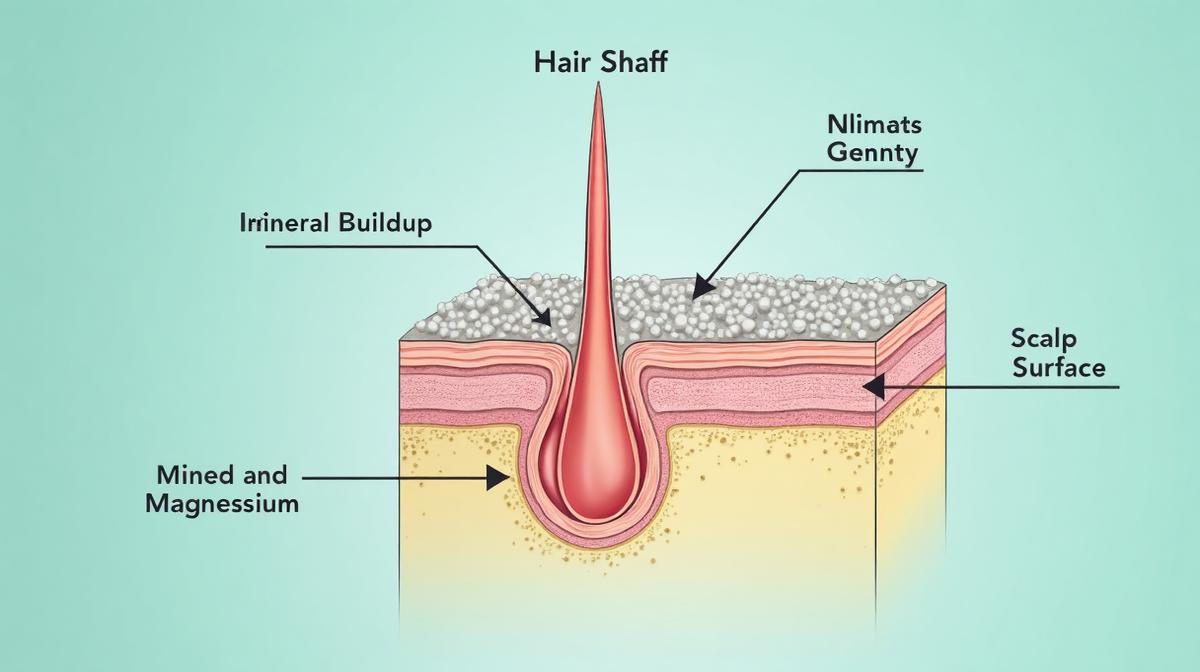
Teenagers in the Gulf face unique environmental stressors that compound normal adolescent hair challenges. Hard water with high mineral content is ubiquitous across the region. While hard water doesn’t directly cause hair loss, it creates scalp conditions that worsen existing problems.
Mineral deposits from hard water build up on the scalp, creating a barrier that blocks topical treatments and traps sebum. For teenagers already dealing with hormonal sebum overproduction, this creates a perfect environment for inflammation and folliculitis. The result: itchy, inflamed scalp that changes normal hair growth.
Indoor air conditioning runs constantly in Gulf homes and schools, creating low-humidity environments (often 20-30% relative humidity). Dry air dehydrates hair shafts, increases breakage, and makes existing thinning more noticeable. Teenagers with naturally curly or textured hair are particularly affected.
Sun exposure, despite being limited due to climate, still affects hair when teenagers are outdoors. UV radiation degrades hair protein structure and fades natural pigment. Combined with chlorine exposure from swimming pools, this creates brittle, damaged hair that breaks easily.
For teenagers experiencing hair shedding in the Gulf, addressing water quality can improve scalp health even if it doesn’t stop the underlying hair loss. A chelating shampoo like Regrowth+ removes mineral buildup, allowing the scalp to function normally while underlying nutritional or hormonal issues are addressed.
The environmental stressors don’t cause adolescent hair loss, but they make recovery slower and more difficult. Teenagers dealing with telogen effluvium or nutritional deficiency need optimal scalp conditions to support regrowth. In the Gulf, that means actively managing water quality and humidity.
Treatment Approaches and Realistic Timelines
Most teenage hair loss is reversible. But recovery takes time, and expectations need calibration. Hair grows approximately 1cm per month. If a teenager lost 40% of hair density over 4 months, regrowth to baseline takes 8-12 months minimum.
For nutritional deficiencies, treatment starts with supplementation at therapeutic doses. Iron deficiency requires 65mg elemental iron daily for 3-6 months until ferritin reaches 70-80 ng/mL. Vitamin D deficiency needs 2000-4000 IU daily for 8-12 weeks, then maintenance. B12 deficiency may require sublingual or intramuscular supplementation if absorption is impaired.
Hormonal causes (PCOS, thyroid disorders) require endocrinology consultation and specific medical management. Birth control pills help some teenage girls with PCOS-related hair loss by reducing androgen levels. Thyroid medication normalizes hair growth in hypothyroid teenagers within 4-6 months.
Minoxidil is FDA-approved for ages 18 and up, but pediatric dermatologists sometimes prescribe it off-label for younger teenagers with significant androgenetic alopecia. The 2% solution is typically used in adolescents. Response takes 4-6 months to become visible.
For stress-related telogen effluvium, no medication is necessary. The hair regrows spontaneously once the stressor resolves or the teenager adapts. The challenge is convincing anxious teenagers (and parents) that doing nothing is appropriate. Unnecessary treatments create more stress and potentially worsen shedding.
Trichotillomania requires cognitive behavioral therapy, specifically habit reversal training. Medication (SSRIs) may help if underlying anxiety or OCD is present. Hair regrows normally once pulling stops, but relapse is common without sustained behavioral intervention.
Realistic timeline for most reversible teenage hair loss: 3 months to stop shedding, 6 months to see new growth, 12 months to return to baseline density. Faster recovery is rare. Slower recovery suggests an unaddressed underlying cause.
References
- Hormonal Effects on Hair Follicles During Puberty - Journal of Clinical Endocrinology & Metabolism
- Hair Loss in Adolescents with Eating Disorders - International Journal of Eating Disorders
- Serum Ferritin and Hair Loss: A Quantitative Study - Journal of the American Academy of Dermatology
- Trichotillomania in Children and Adolescents - American Academy of Dermatology