This article contains affiliate links. See our affiliate disclosure for details.
Your dermatologist pulls out what looks like a small magnifying device, places it against your scalp, and suddenly you’re both staring at a screen showing your hair follicles at 50x magnification. Welcome to trichoscopy, the diagnostic tool that’s changed how we diagnose hair loss.
It’s not new technology. Dermoscopy has been used in dermatology for decades, primarily for examining skin lesions. But its application to scalp and hair disorders, trichoscopy, has only become standard practice in the last 15 years. What makes it valuable isn’t just the magnification. It’s what that magnification reveals: patterns invisible to the naked eye that distinguish androgenetic alopecia from alopecia areata, telogen effluvium from scarring alopecias, and even environmental damage from genetic conditions.
Here’s what happens during the exam, what it can and can’t tell you, and when it’s worth asking your doctor for one. Because if you’ve been losing hair in the Gulf region and standard blood tests came back normal, trichoscopy might reveal what’s actually happening at the follicle level, including mineral buildup that standard exams miss.
What Trichoscopy Actually Shows
Trichoscopy uses a handheld dermoscope, a device with polarized light and magnification ranging from 10x to 70x, to examine the scalp surface and hair shafts. The polarized light penetrates the outer layers of skin, revealing structures and patterns that aren’t visible otherwise.
What you’re looking at isn’t just “zoomed in hair.” You’re seeing follicular units (groups of 1-4 hairs emerging from a single follicle opening), the diameter variation between hair shafts, the scalp’s vascular patterns, pigmentation irregularities, and surface deposits. These patterns are diagnostic.
In androgenetic alopecia (pattern hair loss), trichoscopy reveals hair shaft miniaturization, the progressive thinning of individual hairs. You’ll see a mix of thick terminal hairs and progressively thinner vellus-like hairs emerging from the same area. The ratio of thin to thick hairs increases in affected zones. You’ll also see increased spacing between follicular units and yellow dots (sebum-filled follicle openings) where hairs have been lost.
In alopecia areata (autoimmune hair loss), the signature findings are exclamation mark hairs (broken hairs that taper at the base), black dots (remnants of broken hairs within the follicle), and yellow dots in acute patches. The pattern is distinct from androgenetic alopecia because there’s no gradual miniaturization, hairs are either present or broken off.
In telogen effluvium (diffuse shedding), trichoscopy shows a higher percentage of empty follicle openings and uniform hair shaft diameter without miniaturization. The key finding is that the hairs you still have aren’t getting thinner, they’re just fewer in number temporarily.
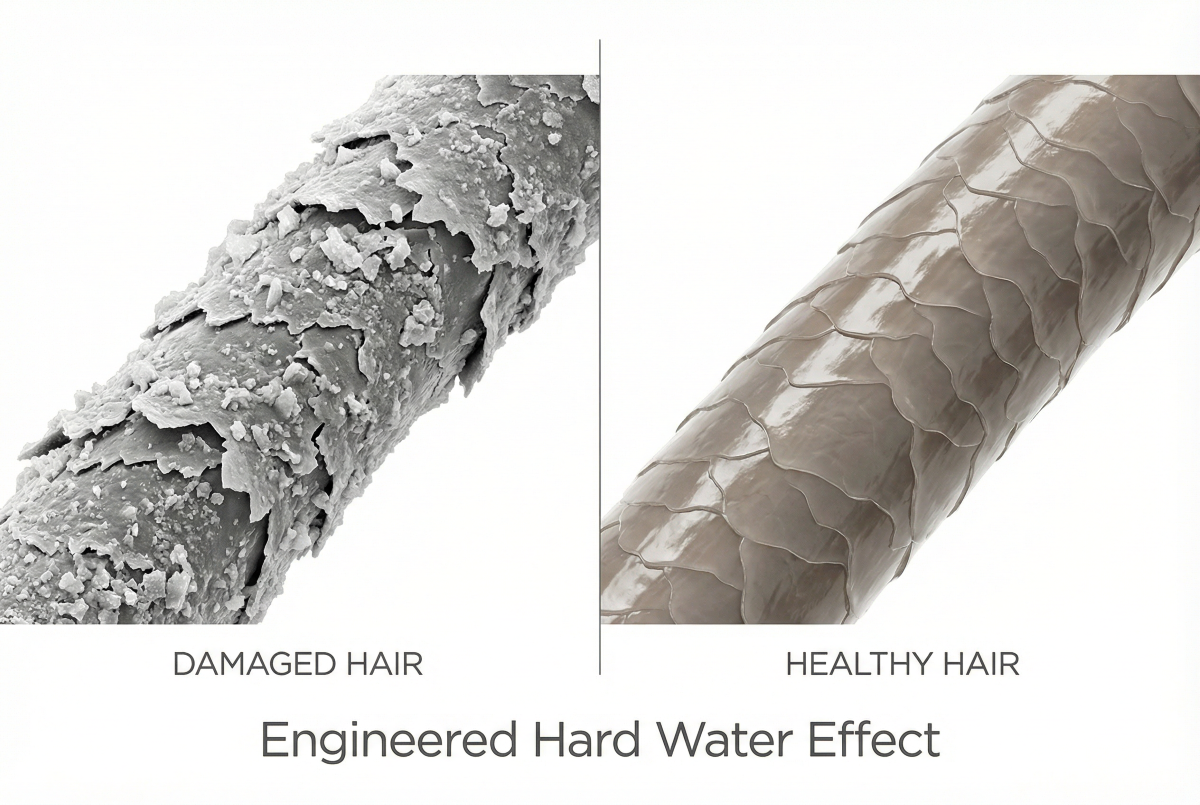
And here’s what surprises many patients: trichoscopy can reveal environmental damage. In regions with hard water, you’ll see white or yellowish deposits coating hair shafts and accumulating around follicle openings. A 2019 study in the International Journal of Trichology documented these mineral deposits as a distinct trichoscopic finding in patients with hard water exposure, separate from genetic hair loss patterns.
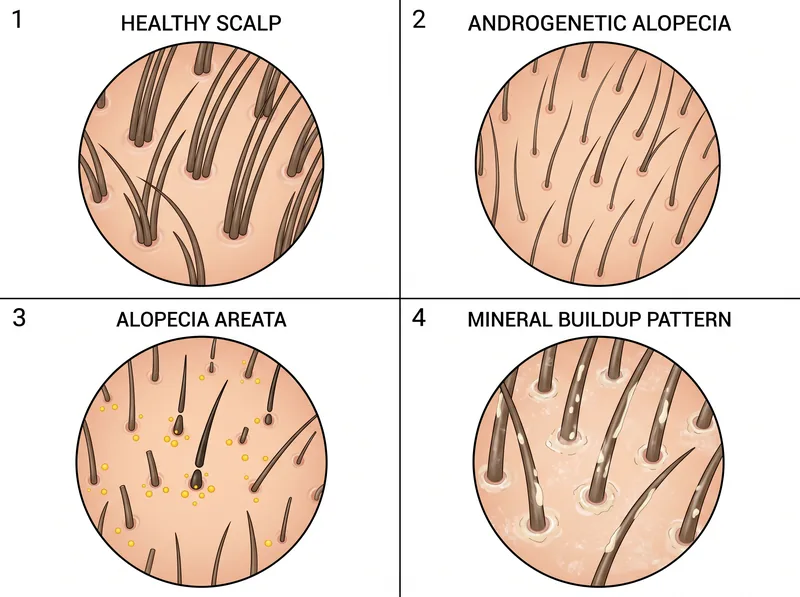 Trichoscopy reveals distinct patterns: healthy follicles show consistent density, androgenetic alopecia displays miniaturization, alopecia areata shows exclamation mark hairs, and hard water damage reveals mineral deposits coating hair shafts.
Trichoscopy reveals distinct patterns: healthy follicles show consistent density, androgenetic alopecia displays miniaturization, alopecia areata shows exclamation mark hairs, and hard water damage reveals mineral deposits coating hair shafts.
The Examination Process
The exam itself takes 10-15 minutes. You don’t need to wash your hair beforehand, in fact, some dermatologists prefer you don’t, because natural sebum distribution and any surface buildup are part of what they’re assessing.
Your dermatologist will examine multiple zones: the frontal hairline, vertex (crown), temporal areas, and occipital (back) region. They’re comparing patterns between affected and unaffected areas. In androgenetic alopecia, for example, the occipital region typically shows normal follicular density even when the vertex is severely affected. That comparison is diagnostic.
The dermoscope is placed directly against your scalp, usually with a contact gel or immersion fluid to improve visualization. Some newer devices are non-contact and use polarized light without gel. Images are captured digitally, which allows for documentation and comparison over time, critical for tracking treatment response.
What you’re seeing on the screen is real-time. Your dermatologist will often narrate what they’re observing: “Here’s miniaturization in the frontal zone. See how these three hairs are different diameters? That’s progressive miniaturization. Now look at the back, uniform diameter, normal density. Classic androgenetic pattern.”
The exam is completely non-invasive. No needles, no tissue removal, no discomfort beyond having someone part your hair and press a device against your scalp. If your scalp is sensitive or inflamed, they’ll work around it.
What Trichoscopy Can’t Diagnose
Trichoscopy is a surface exam. It shows you what’s happening at the follicle opening and along the visible hair shaft, but it doesn’t reveal what’s happening inside the follicle or beneath the scalp surface. For that, you’d need a scalp biopsy, a more invasive procedure where a small tissue sample is removed and examined under a microscope.
It can’t definitively diagnose scarring alopecias (conditions where follicles are permanently destroyed) without biopsy confirmation. Trichoscopy can show findings suggestive of scarring, loss of follicle openings, fibrosis, altered pigmentation, but the gold standard for diagnosing lichen planopilaris, frontal fibrosing alopecia, or discoid lupus is still histopathology.
It can’t measure hormone levels, nutrient deficiencies, or thyroid function. If your hair loss is driven by low ferritin, B12 deficiency, or thyroid dysfunction, trichoscopy will show the resulting pattern (often diffuse thinning without miniaturization) but won’t identify the underlying cause. You still need blood work.
It can’t predict future progression with certainty. Trichoscopy shows the current state of your follicles, but whether your androgenetic alopecia will progress rapidly or slowly depends on genetics, hormones, and environmental factors that the exam can’t measure. It’s a snapshot, not a forecast.
And it can’t distinguish between temporary and permanent damage in all cases. Mineral buildup from hard water is visible on trichoscopy, but whether the follicles underneath are temporarily suppressed or permanently miniaturized requires follow-up exams after the environmental factor is addressed. That’s why dermatologists often recommend a chelating shampoo like Regrowth+ to remove surface deposits before repeating the exam three months later.
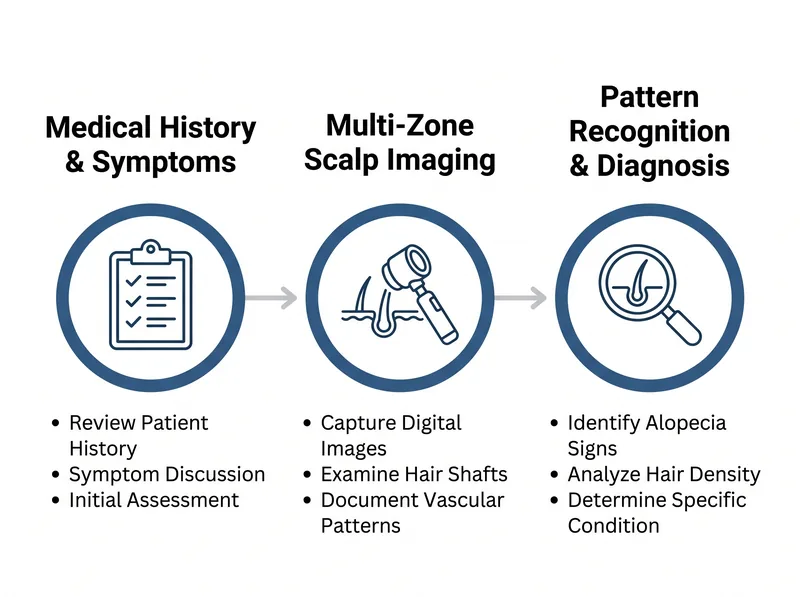 The diagnostic process: consultation establishes history, trichoscopy examination captures magnified images of multiple scalp zones, and analysis identifies specific patterns that point to underlying causes.
The diagnostic process: consultation establishes history, trichoscopy examination captures magnified images of multiple scalp zones, and analysis identifies specific patterns that point to underlying causes.
When to Ask for Trichoscopy
If you’re experiencing hair loss and your doctor is relying solely on visual inspection and medical history, ask about trichoscopy. It’s increasingly available outside specialist clinics, many general dermatologists now have dermoscopes in their offices.
You should specifically request it if you’ve had normal blood work but ongoing hair loss. Standard labs can miss subclinical deficiencies, and trichoscopy can reveal whether the problem is follicular miniaturization (suggesting androgenetic alopecia or DHT sensitivity) or diffuse shedding without miniaturization (suggesting telogen effluvium from stress, nutrition, or environmental factors).
Request it if you’ve recently moved to the Gulf region and developed sudden hair changes. Trichoscopy can show mineral deposits coating your hair shafts and scalp surface, a finding that points directly to hard water exposure rather than genetic hair loss. That distinction changes your entire treatment approach.
Ask for it before starting minoxidil or finasteride. Baseline trichoscopic images document your starting point, making it possible to objectively measure treatment response six months later. A 2017 study in the Journal of the American Academy of Dermatology found that trichoscopy-guided treatment decisions improved patient outcomes because doctors could distinguish responders from non-responders early and adjust protocols.
And request it if you’ve been diagnosed with androgenetic alopecia but aren’t responding to standard treatments. Trichoscopy can reveal whether you actually have androgenetic alopecia or a different condition that mimics it, like chronic telogen effluvium, diffuse alopecia areata, or environmental damage masquerading as genetic loss.
Interpreting Your Results
Your dermatologist should walk you through the images and explain what they’re seeing. If they don’t, ask. The patterns are visual and relatively straightforward once you know what to look for.
Hair shaft diameter variation is the key finding in androgenetic alopecia. If you see thick hairs next to progressively thinner hairs in the same follicular unit, that’s miniaturization. The more variation, the more advanced the androgenetic component. If all your hairs are roughly the same diameter, androgenetic alopecia isn’t the primary driver.
Yellow dots (sebaceous glands visible through empty follicle openings) indicate follicles that have stopped producing terminal hairs. A few scattered yellow dots are normal. Clusters of them in the frontal or vertex region suggest advanced androgenetic alopecia. In alopecia areata, yellow dots appear suddenly in patches rather than gradually across a zone.
White or yellowish deposits on hair shafts and around follicles indicate surface buildup, usually from hard water minerals, styling products, or sebum oxidation. These deposits don’t cause hair loss directly, but they create a coating that can interfere with topical treatments and exacerbate scalp inflammation in sensitive individuals.
Vascular patterns (the tiny blood vessels visible beneath the scalp surface) can indicate inflammation. Increased, dilated, or irregular vessels suggest an active inflammatory process, common in scarring alopecias, severe seborrheic dermatitis, or autoimmune conditions. Normal, fine vascular networks are a reassuring finding.
Cost and Accessibility in the Gulf
Trichoscopy is typically included in a dermatology consultation fee, you’re not paying separately for the exam itself. In the Gulf region, expect consultation fees ranging from 300-800 AED (roughly $80-220 USD) depending on the clinic and whether you’re seeing a general dermatologist or a trichology specialist.
Most insurance plans cover dermatology consultations for medical concerns (hair loss qualifies), but coverage for trichoscopy specifically varies. Check with your provider. If you’re paying out of pocket, the exam adds negligible cost, the dermoscope is a standard tool, not a specialized billable procedure.
Availability is good in major Gulf cities. University hospital dermatology departments, private dermatology clinics, and dedicated hair restoration centers typically offer trichoscopy. Smaller clinics may not have the equipment, so call ahead and ask whether the dermatologist performs trichoscopic examinations.
If your first dermatologist doesn’t offer trichoscopy and you feel it would be valuable (especially if you’ve had inconclusive results from standard exams), it’s reasonable to seek a second opinion at a clinic that does. The exam provides objective data that can resolve diagnostic uncertainty.
Some clinics offer trichoscopy as part of a complete hair loss evaluation package that includes blood work, scalp biopsy (if needed), and follow-up exams. These packages typically run 1500-3000 AED ($400-800 USD) and can be worthwhile if you’re dealing with complex or treatment-resistant hair loss.
References
- Trichoscopy in hair disorders: A complete review - International Journal of Trichology
- Dermoscopy of the scalp: A review of findings in inflammatory and infectious scalp diseases - Journal of the American Academy of Dermatology
- Trichoscopy: How it may help in diagnosis and monitoring of hair and scalp disorders - PubMed Central
- Dermoscopy in general dermatology: A practical overview - American Academy of Dermatology