This article contains affiliate links. See our affiliate disclosure for details.
You’ve noticed the thinning. You’ve tried the over-the-counter solutions. Now you’re sitting in a waiting room, about to see a dermatologist for the first time about your hair loss. Your mind is racing with questions you should’ve written down.
Here’s the thing: most people walk into their first hair loss consultation unprepared. They forget crucial details. They don’t ask the right questions. And they leave with more confusion than clarity.
This isn’t your fault. Medical appointments are intimidating, and hair loss is emotionally charged. But the quality of your diagnosis depends entirely on the information you provide and the questions you ask. A dermatologist can’t read your mind or your medical history from a five-minute scalp exam.
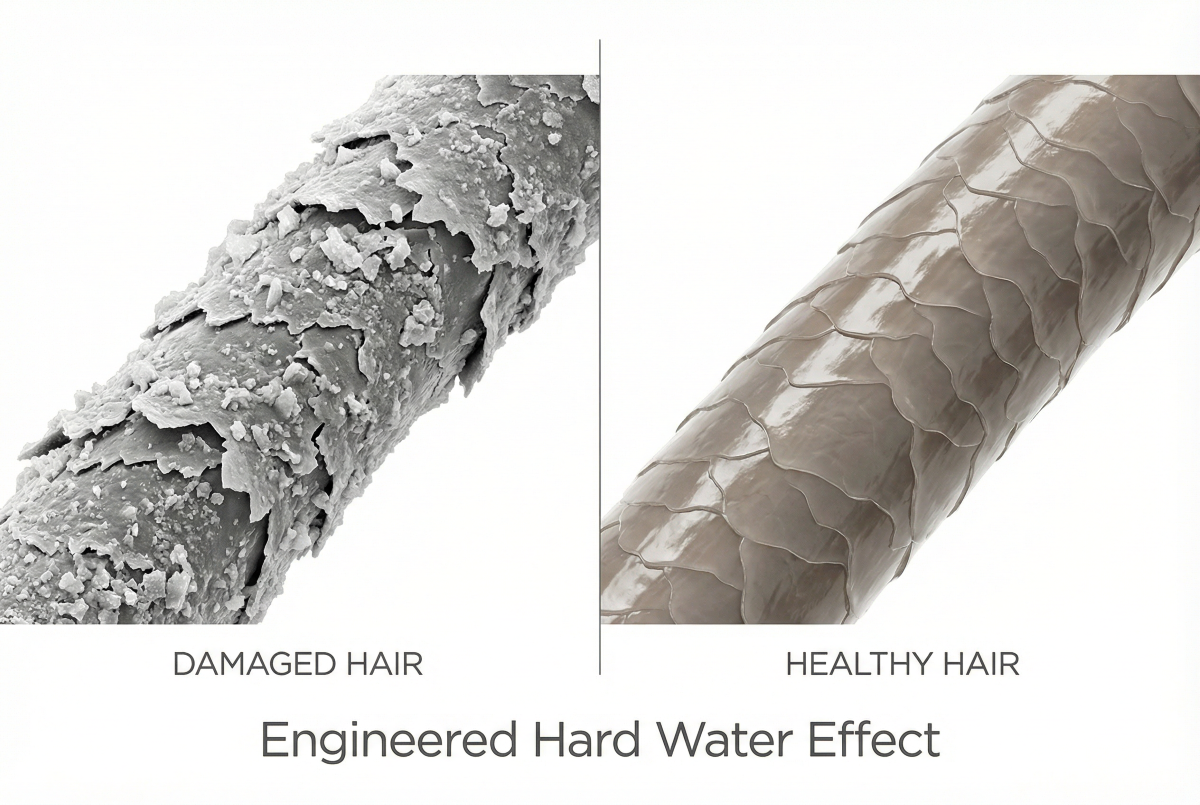
This guide walks you through exactly what to bring, what to ask, and how to describe your symptoms so you get the most accurate diagnosis possible. Whether you’re experiencing gradual thinning or sudden shedding, preparation makes the difference between a generic recommendation and a targeted treatment plan. For residents in the Gulf region, environmental factors like hard water exposure add another layer worth discussing with your specialist.
What to Bring to Your Appointment
Walk in with documentation, not just descriptions. Your dermatologist needs concrete data to identify patterns that might not be obvious from a single examination.
Bring photos showing your hair at different time points. Not artistic selfies, clinical documentation. Take photos in the same lighting, from the same angles: front hairline, crown, part line. Monthly photos over three to six months reveal progression that’s invisible day-to-day. If you’ve been losing hair for years but only have recent photos, bring what you have. Something is better than nothing.
Compile a list of every medication and supplement you’ve taken in the past year. Include dosages and start dates. Many drugs cause hair loss as a side effect, but the shedding doesn’t start immediately. Telogen effluvium from medications can begin two to four months after you start a new prescription. Your dermatologist needs to see the timeline.
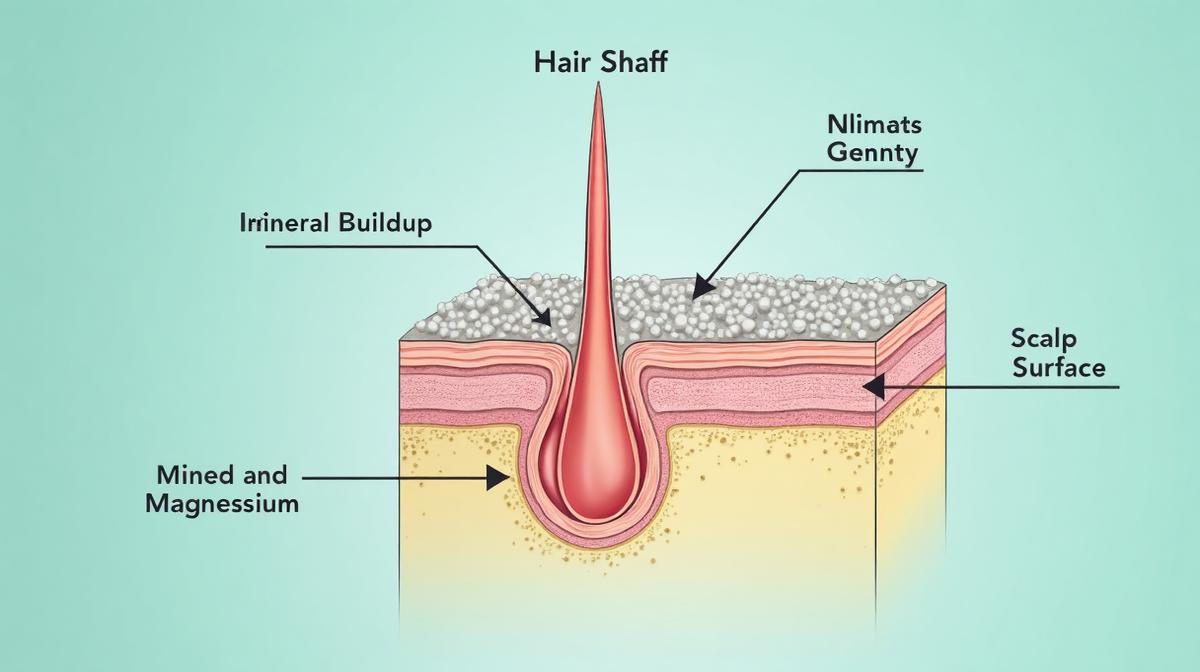
Document your hair care routine. What shampoo do you use? How often? Do you use heat styling tools? Chemical treatments? Hair extensions? For Gulf residents, note if you’ve recently moved to the region or changed your water filtration system. Hard water mineral buildup can mimic or worsen hair loss symptoms, and a chelating shampoo like Regrowth+ may be recommended as part of your scalp preparation routine.
Bring recent bloodwork if you have it. Ferritin, thyroid panels, vitamin D, B12, these are standard tests for hair loss, and having recent results saves time. If you don’t have bloodwork, expect your dermatologist to order it. Ferritin levels below 40 ng/mL can cause shedding even when they’re technically “normal” by lab standards.
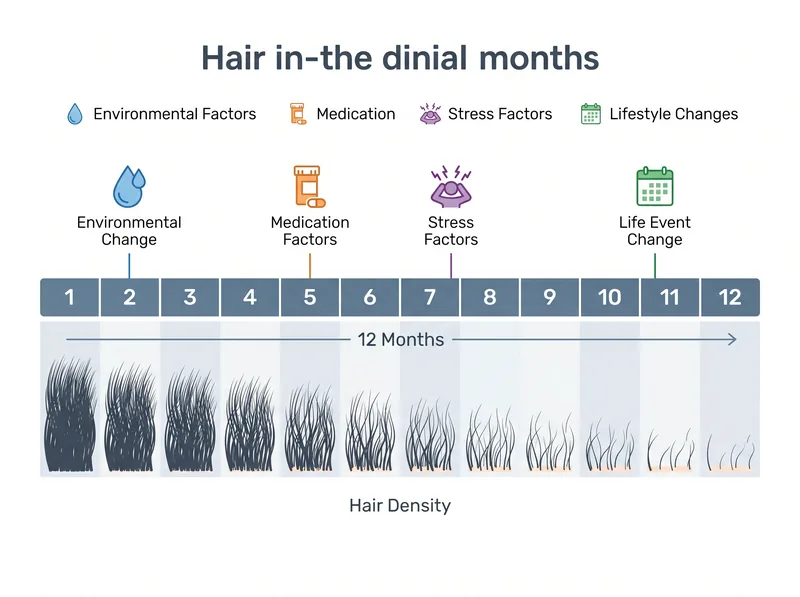 Documenting your hair loss timeline helps your dermatologist identify patterns and potential triggers
Documenting your hair loss timeline helps your dermatologist identify patterns and potential triggers
How to Describe Your Symptoms Accurately
Vague descriptions lead to vague diagnoses. “My hair is falling out” doesn’t tell your dermatologist what they need to know. Be specific about the pattern, timeline, and characteristics of your hair loss.
Describe where you’re losing hair. Is it diffuse thinning across the entire scalp? Concentrated at the hairline? A widening part? Patchy bald spots? Different patterns indicate different causes. Androgenetic alopecia follows a predictable pattern, receding temples and crown thinning in men, widening part in women. Telogen effluvium causes diffuse shedding. Alopecia areata creates circular patches.
Quantify the shedding if possible. How many hairs do you see in the shower drain? On your pillow? When you run your fingers through your hair? Normal shedding is 50-100 hairs per day, but most people can’t count that accurately. Instead, compare to your baseline: “I used to clean the drain once a week, now it’s daily.” That’s useful information.
Note any changes in hair texture. Is your hair thinner in diameter? More brittle? Less shiny? Texture changes often precede visible thinning and can indicate miniaturization of the hair follicle, a hallmark of androgenetic alopecia.
Mention associated symptoms. Scalp itching, burning, redness, flaking, or tenderness all point to specific conditions. Seborrheic dermatitis, folliculitis, and scalp psoriasis can all cause hair loss, but they require different treatments than pattern baldness. Don’t assume symptoms are unrelated.
Essential Questions About Diagnosis and Testing
Your dermatologist will examine your scalp, but you need to understand what they’re looking for and what tests they’re considering. Don’t leave the office without clarity on these points.
Ask: “What type of hair loss do I have?” There are over a dozen types of alopecia, and the treatment for one won’t work for another. You need a specific diagnosis, not just “hair loss.” If your dermatologist says “telogen effluvium,” ask what triggered it. If they say “androgenetic alopecia,” ask about the severity stage.
Ask: “What tests do you recommend and why?” Bloodwork is standard, but scalp biopsies and trichoscopy provide additional diagnostic value in ambiguous cases. Understand what each test reveals and whether it’s necessary for your situation.
Ask: “Could this be temporary or reversible?” Not all hair loss is permanent. Telogen effluvium from stress, illness, or nutritional deficiency often resolves once the trigger is addressed. Androgenetic alopecia is progressive but can be slowed or partially reversed with treatment. Knowing the prognosis helps you set realistic expectations.
Ask: “What’s causing this?” Don’t accept “genetics” as the full answer. Even genetic hair loss has triggers and accelerating factors. Environmental stress, nutritional deficiencies, hormonal changes, these all interact with genetic predisposition. Understanding your specific contributing factors guides treatment strategy.
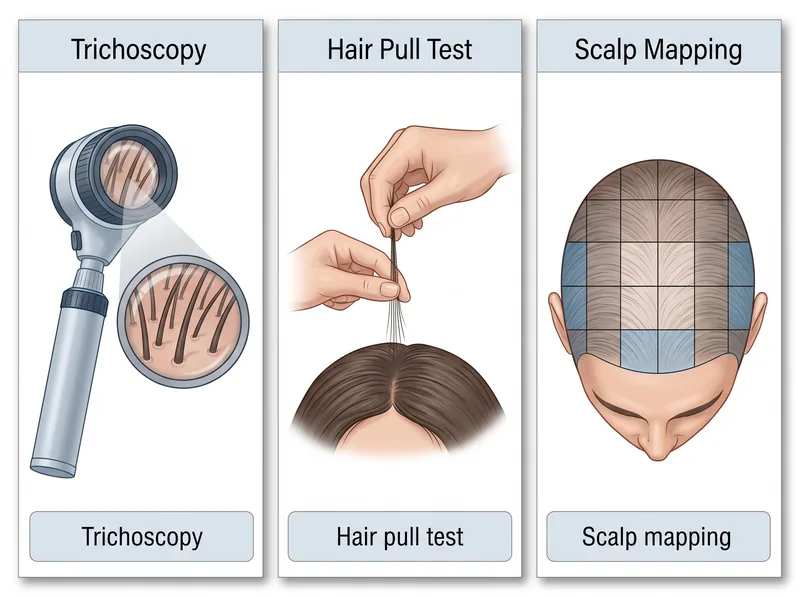 Understanding common examination methods helps you know what to expect during your appointment
Understanding common examination methods helps you know what to expect during your appointment
Treatment Options and What to Expect
Once you have a diagnosis, the conversation shifts to treatment. This is where many patients get overwhelmed by options and conflicting information. Ask structured questions to understand the evidence, timeline, and commitment required.
Ask: “What are my treatment options, and what’s the evidence for each?” For androgenetic alopecia, the FDA-approved options are minoxidil and finasteride (men) or minoxidil and spironolactone (women). Everything else is either off-label or unproven. Low-level laser therapy has some evidence, but it’s expensive and requires consistent use. Understand what’s backed by clinical trials versus what’s marketed hype.
Ask: “How long until I see results?” Hair growth is slow. Minoxidil takes three to six months to show improvement. Finasteride can take six to twelve months. If your dermatologist promises visible results in weeks, be skeptical. Realistic timelines prevent premature treatment abandonment.
Ask: “What are the side effects and how common are they?” Every treatment has risks. Finasteride can cause sexual side effects in a small percentage of men. Minoxidil can cause scalp irritation and unwanted facial hair growth in women. Spironolactone affects blood pressure and potassium levels. You need to know what to monitor and when to be concerned.
Ask: “What happens if I stop treatment?” Most hair loss treatments require indefinite use. Stop minoxidil, and you’ll lose the regrown hair within months. Stop finasteride, and androgenetic alopecia progression resumes. This isn’t a failure of the treatment, it’s the nature of the condition. Understanding the commitment upfront prevents frustration later.
Ask: “Should I address environmental factors first?” If you live in the Gulf and have hard water exposure, mineral buildup on the scalp can interfere with treatment absorption and worsen inflammation. Some dermatologists recommend improving scalp health before starting medications to improve treatment response.
Lifestyle and Environmental Factors to Discuss
Your hair doesn’t exist in a vacuum. Diet, stress, sleep, water quality, these all affect hair health. Many dermatologists focus on medical treatment and skip the lifestyle conversation, so you need to bring it up.
Ask: “Could my diet be contributing?” Protein deficiency, low zinc, B12 deficiency, these are common in restrictive diets and can cause telogen effluvium. If you’re vegetarian, vegan, or following a low-calorie diet, mention it. Your dermatologist should assess whether nutritional supplementation is warranted.
Ask: “How does stress affect my hair loss?” Chronic stress doesn’t directly cause androgenetic alopecia, but it can trigger telogen effluvium and accelerate existing hair loss. Stress hormones affect the hair growth cycle, and managing stress can improve treatment outcomes. Don’t dismiss this as irrelevant.
Ask: “Could water quality be a factor?” For Gulf residents, this is critical. Hard water in the GCC has extremely high mineral content that deposits on the scalp, clogs follicles, and creates inflammation. If you’ve noticed increased shedding after moving to the region, mention it. Your dermatologist may recommend water testing or filtration solutions.
Ask: “Are there hairstyles or products I should avoid?” Traction alopecia from tight hairstyles is preventable but permanent if caught too late. Chemical relaxers, bleach, and heat styling all damage the hair shaft. If you’re already experiencing hair loss, additional mechanical or chemical stress makes it worse.
Follow-Up and Monitoring Your Progress
Hair loss treatment isn’t a one-time prescription. It requires monitoring, adjustments, and realistic progress tracking. Establish the follow-up plan before you leave the office.
Ask: “When should I come back for a follow-up?” Most dermatologists schedule reassessment at three to six months, which aligns with the hair growth cycle. If you’re starting a new treatment, you need a follow-up to assess response and side effects. Don’t wait until you’ve decided the treatment “isn’t working” to make another appointment.
Ask: “How will we measure progress?” Subjective assessment (“Does my hair look thicker?”) is unreliable. Some dermatologists use standardized photography, hair counts, or trichoscopy to track changes objectively. Knowing the measurement method helps you understand whether you’re actually improving or just hoping.
Ask: “What signs should prompt me to call before my scheduled follow-up?” Severe side effects, sudden increase in shedding, scalp pain or infection, these warrant earlier contact. Understand what’s normal treatment response versus what requires immediate attention.
Ask: “Can I contact you with questions between appointments?” Some dermatologists offer patient portal messaging or nurse consultation lines. Knowing how to reach your provider prevents unnecessary anxiety and ensures you’re using treatments correctly.
References
- Drug-induced hair loss: A complete review - PubMed
- Types of Hair Loss - American Academy of Dermatology
- The Role of Vitamins and Minerals in Hair Loss: A Review - PubMed Central
- Efficacy and Safety of Low-level Laser Therapy for Androgenetic Alopecia - PubMed
- Stress and the Hair Growth Cycle - PubMed Central